
A Patient with Isolated Hand Weakness
Elisabeth B. Lucassen*, Aiesha Ahmed
Affiliation
Department of Neurology, Penn State University, Hershey, PA, USA
Corresponding Author
Elisabeth Lucassen. Department of Neurology, Penn State University, Hershey, PA, USA. Tel: 717-531-1804; Fax: 717-531-4694; E-mail: elucassen@hmc.psu.edu
Citation
Lucassen, B. E., et al. A Patient with Acute Isolated Hand Weakness Due To Cortical Ischemic Damage.(2015) Int J Neurol Brain Disord 2(2): 1- 2.
Copy rights
© 2015 Lucassen, B. E. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Hand knob syndrome; Stroke; Weakness
Abstract
Small cortical strokes can produce symptoms mimicking those from peripheral nerve diseases. In cases where the presentation is sudden in onset and limited to monparesis of a limb, especially affecting the distal muscles, the diagnosis of a central nervous system lesion should be considered.
Introduction
Clinical Presentation
A 57-year-old woman presented with a two-day history of right hand weakness. The onset was sudden and was not preceded by trauma. There was no numbness and associated pain noted by the patient. She denied any neck pain at the time of presentation as well in the recent past. She had past medical history significant for hypertension and hyperlipidemia. No concurrent difficulty with speech, swallowing, coordination and incontinence was noted by the patient. She denied weakness elsewhere.
On examination, she had normal mental status. Her cranial nerves were all intact. Speech was fluent without any dysarthria. The motor exam showed full strength symmetrically in all muscle groups except for the right hand finger flexion and interossei where strength was graded as 4/5. Reflexes were symmetrically 2+. Sensory exam was symmetrically intact to pinprick, vibration and position sense. Her casual gait was normal. No dysmetria or apraxia was noted.
Her basic labs were normal. The electrocardiogram and transthoracic echocardiogram were unremarkable. Imaging was ordered due to the acuteness of the presentation. A brain MRI diffusion weighted (Figure 1, Image A) and Apparent Diffusion Coefficient (Figure 1, Image B) revealed abnormalities in the left precentral gyrus. High Signal intensity in this region is also seen on the FLAIR (Figure 1, Image C) and T2-weighted (Figure 1, Image D) sequences. MRA of intracranial vessels was unrevealing. Carotid ultrasound studies showed ipsilateral extracranial internal carotid artery (ICA) stenosis of 50%.
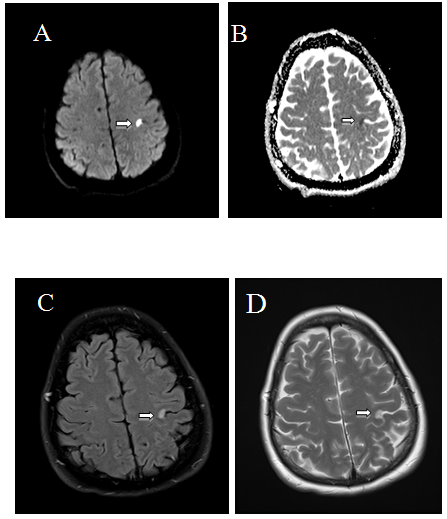
Figure 1A: CT scan of the head on presentation showing Right frontal peripherally enhancing centrally necrotic lesion with slight right-to-left subfalcine herniation approximately 0.3 cm.
Discussion
It has been shown that the cortical representation of motor hand function is located in the superior part of the precentral gyrus[1]. Isolated weakness of the fingers may be prominent in either radial-sided or ulnar-sided fingers with infarcts in the precentral gyrus or “hand knob”[2]. As the finger paralysis caused by a cortical lesion can be partial, with only a few fingers involved, this can also produce the so-called pseudoradicular pattern[3].
Monoparesis caused by cerebral insult is rare and is more often caused by mass lesions such as a tumor or abscess rather than by vascular damage[3,4] MRI can be helpful in determining the underlying CNS etiology. In this case, the patient’s presentation was acute, which would be suspicious for a stroke and less typical for a peripheral nerve lesion. As such, it is important to have a broad differential when evaluating a patient with acute isolated hand weakness as this would change the management of the patient.It is possible that hypertension and atherosclerosis leading to an arterio-arterial thrombembolic stroke mechanism was the etiology of stroke in our patient.
References
- 1. Han, Y.S., Ha, S.W., Cho, J.S., et al. Isolated Weakness of Middle, Ring, and Little Fingers due to a Small Cortical Infarction in the Medial Precentral Gyrus. (2006) J Clin Neurol 2(2): 146- 148.
- 2. Kim, J.S., Chung, J.P., Ha, S.W. Isolated weakness of index finger due to small cortical infarction. (2002) Neurology 58(6):985.
- 3. Takahashi, N., Kawamura, M., Araki, S. Isolated hand palsy due to cortical infarction: localization of the motor hand area. (2002) Neurology 58(9):1412- 1414.
- 3. Granziera, C., Kuntzer, T., Vingerhoets, F., et al. Small cortical stroke in the “hand knob” mimics anterior interosseous syndrome. (2008) J Neurol 255(9): 1423- 1424.










