
A Retrospective Analysis of Outcome following Neuronavigation Guided Trans-Nasal, Trans-Sphenoidal Microscopic Excision of Pituitary Tumors: Study at Khoula Hospital of Cases Operated Between 2009 and 2017.
Munthir Al-ZabinAli M. Al-Mashani1, MunthirJ. M. Al-Zabin1*, Neeraj Salhotra1, Maimuna S N Al Saadi1, Azmat Ali1
Affiliation
1Department of Neurosurgery, Khoula Hospital, Sultanate of Oman, Muscat
2Department of Histopathology, Khoula Hospital, Sultanate of Oman, Muscat
Corresponding Author
Dr. Munthir Al-Zabin, MD, PhD, Sr. Specialist, Department of Neurosurgery, Khoula Hospital, Sultanate of Oman, Muscat; E-mail: munthir.alzabin@yahoo.com
Citation
Al-Zabin, M., et al. A Retrospective Analysis of Outcome Following Neuronavigation Guided Trans-Nasal, Trans-Sphenoidal Microscopic Excision of Pituitary Tumors: Study at Khoula Hospital of Cases Operated Between 2009 and 2017. (2018) Int J Neurol Brain Dis 5(1): 1- 5.
Copy rights
© 2018 Al-Zabin, M. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Pituitary tumors; Neuro-navigation; Trans-nasal trans-sphenoidal approach; Pituitary tumor apoplexy; Dopamine-agonist; Micro- and macroadenoma
Abstract
This is a 7-year retrospective analysis with the primary objective of noting the incidence of pituitary tumor recurrence after transnasal trans-sphenoidal approach using neuronavigation and operating microscope under a single operating unit. The secondary objective was to identify the type of tumor with highest secretory over activity and operative complications. The follow up period ranged between one to seven years.
The result of this analysis of 67 patients indicates that the tumor size ranged between 5.7 X 5.7 mm to 49.5 X 35.5 mm. Headache was the commonest presenting symptom in 83.6% cases.The incidence of functioning adenomas in this series was 80.5% with prolactin being the dominant over secretory hormone in 53.7% cases. We noted an overall recurrence rate of 17.9%. The most important complication was a CSF leak noted in 11 patients (16.4%). CSF leak was fully cured in all patients by using a lumbar drainage catheter and/or placement of fat at the leakage site. There was only one mortality is this series.
Introduction
The worldwide incidence of primary central nervous system (CNS) tumors, age-adjusted using the world standard population, is 7.5 - 19.3 per 100,000 person-years[1,2]. The incidence of pituitary tumors in the general population among the CNS tumors has been quoted to range between 10 - 16.7%[1,2]. They are often symptomless benign adenomas but when the tumor size exceeds 10 mm (macroadenoma), it often results in visual field disturbances, compression of cranial nerves, hypopituitarism, and infiltration of the cavernous sinuses[3]. Though surgery produces a quick reversal of patient’s symptoms but 24 - 61% patients were noted to have recurrence when evaluated at two academic centers in France and Belgium[4]. Unfortunately, Brochier et al, 2010[4] did not state whether the surgery was done using operating microscope, neuronavigation or any other advanced operating aids at these two centers. Roelfsema et al[5] analyzed data about pituitary adenomas from 143-publications upto 2012. They reported that 95% of these publications were based on surgery done using only operating microscope, without additional aids such as neuronavigation, endoscope or intraoperative MRI.
At our center, one of the neurosurgery units operated all except three pituitary adenomas since 2009 via trans-sphenoidal trans-nasal (TSTN) route using operating microscope and neuronavigation system.We carried out a 7-year retrospective analysis with primary objective of noting the incidence of tumor recurrence and secondarily, identify type of tumor with highest secretory over activity and operative complications.The follow up period ranged between one to seven years.
Materials and Methods
After obtaining permission from Ethical Issues Committee to publish the hospital data, we could retrieve data of 67 consecutive patients who underwent surgery for sellar / intrasellar space occupying lesions (SOL) under a single neurosurgical unit between 2009 and 2017. Operative technique included Neuronavigation guided Neuro-Microscopy and the approach was TSTN for 85 operations in 67 patients; however, 2 operations for recurrence tumors were done by usual craniotomy for pituitary adenomas.
All patients had undergone exhaustive clinical examination and imaging workup prior to surgery including a thorough pre-anesthetic assessment. Patients were explained the advantages and possible complications of the procedure before obtaining written consent.
Intraoperatively, patients were positioned supine with the head held in a 3-pin frame (May field fixation). A slight head elevation and tilting was maintained throughout the operative procedure. Neuronavigation via Brain LABTm (Vector Vision, Germany) was used in all patients.
There were 26 males and 41 females. The mean age was 41.89 yr (range, 17 – 75 yr). There were 59 pituitary adenomas, 2 craniopharyngiomas, 1 empty sella, 1 mucocele, 1 Rathke’s cleft cyst and 3 others (meningioma, glioma, hyperplasia). Pre-operative imaging included MR majority of the cases.
Many of these patients were managed preoperatively with medications prescribed usually by neuro-endocrinologist from the National Centre for Diabetes and Endocrinology.
There were 4 patients where CT scan was the only available imaging. In addition to providing confirmation that a trans-sphenoidal approach was appropriate, the coronal images (MRI or CT) were used to define the position and characteristics of the sphenoid septum, an essential landmark in establishing the position of the midline pre-operatively. Cefuroxime (1.5 g) was administered routinely with induction, together with hydrocortisone (200 mg). Once positioned on the operating table, the anterior nasal mucosa of right nostril was packed with local diluted adrenaline (1:200,000). The face was prepared using aqueous betadine solution / spirit solution, and the right thigh was prepared, in expectation should a fat graft be required.
Surgery was undertaken via the right nostril in all cases using the operating microscope and with guidance of neuronavigation. The sphenoid sinus was approached via a direct transnasal approach. Further access to the sphenoid sinus was obtained via the aditus located high up to the right of the midline. Exposure was then facilitated using pituitary rongeurs or, particularly when the bone was hyperostotic, a small hammer and chisel. After gaining access to the sphenoid sinus, its mucosa was stripped and sent for histopathology and the sella floor opened.
At the conclusion of the procedure, a Valsalva maneuver was performed in all cases. If cerebrospinal fluid (CSF) leakage was evident, then a fat graft was used to seal the sella floor supplemented with tissue glue. In such cases, adjunctive spinal drainage was used for 3 - 5 days postoperatively. Prior to closure, hemostasis was established within the pituitary fossa, often by packing and gentle irrigation with normal saline.
After removing the retractor from the right nostril, a Killian’s retractor was passed into the left side to reposition the septum. Merocel packs were used. Antibiotic prophylaxis was given to all cases for 3 days post-operatively by administering cefuroxime (750 mg) intravenously every 8 hours.
In all cases, the nasal packs were removed on the second post-operative day.
The patient’s management used a well-established post-operative protocol for administration of hydrocortisone, and assessment of endogenous cortisol.
All patients remained in hospital for 5 – 6 days after surgery. The first routine neurosurgical and neuroendocrine clinic follow-up appointment occurred within 4 – 8 weeks of surgery. The patients were subsequently followed up in the clinic for clinical follow up and imaging where necessary.
Results
In this series, the predominant symptoms of the patients were headache (83.6%) followed by visual disturbances (41.8%). Cushingoid features were noted in 14.9% of the patients. Menstrual disturbances in was noted in 13.4% of the cases (Table 1). The correlation of the improvement of the preoperative symptoms, compared with the postoperative symptoms of the patients was statistically significant: Pearson correlation 0.904, P-value = 0.005.
Table 1: Diagnosis and symptoms of the patients.
| Diagnosis Number of patients (%) | Symptoms Number of patients (%) |
|---|---|
| Microadenoma 11 (16.4) | Headache 56 (83.6) |
| Macroadenoma 48 (71.6) | Visual disturbance 28 (41.8) |
| Craniopharyngioma 2 (2.9) | Cushing’s 10 (14.9) |
| Empty sella 1 (1.5) | Menstrual disturbance 9 (13.4) |
| Mucocele 1 (1.5) | Hypertension 5 (7.5) |
| Rathke’s cleft cyst 1 (1.5) | Loss of libido 4 (6.0) |
| Miscellaneous 3 (4.6)-Meningioma, Glioma, Hyperplasia) | Dyslipidemia 3 (4.5) |
| Lactorrhea 3 (4.5) | |
| Psychotic problems 1 (1.5) | |
| Nausea 1 (1.5) | |
| Tinnitus 1 (1.5) | |
| Large breast 1 (1.5) | |
| Facial palsy 1 (1.5) | |
| Proptosis 1 (1.5) | |
| Bitemporal hemianopia 1 (1.5) |
The preoperative diagnostic tool used in this series was noted to be either CT scan (4.4%) or MRI (66.1%). However a mix of both CT and MRI were used in 37.4% of patients.
Laboratory findings established that there were 45 patients (67.2%) who had secretory tumors. Of these, some patients had more than one hormone secretion. The commonest over-secretory hormone was prolactin reported in 36 patients (53.7%) followed by leutinizing hormone in 8 patients (13.4%). One male patient with infertility had increased level of Prolactin and extremely increased level of FSH and a very low level of Testosterone. Of these patients, hormonal levels in serum were normalized or improved in majority of the patients (Table 2).
Table 2: Incidence of tumor recurrence and endocrine status of patients in the pre- and postoperative period.
| Recurrence Tumors (%) | Endocrine laboratory findings (Pre-Op) Number of patients (%) | Endocrine Laboratory findings (Post-op) Number of patients (%) |
|---|---|---|
| Secreting Tumors: Prolactinomas: 5 (7.5%) LH adenomas: 1 (1.5%) | Increased Prolactin level, Prolactinomas: 36 (53.7%) | Prolactinomas: Improved, Hormone WNL 26 (77.0%). proved, Hormone still high 6 (20.0%). No hormonal improvement: 1 (3%) |
| Non secreting tumors: 6 (8.9%) | Increased Luteinizinghormone LH-adenomas: 9 (13.5%) | LH adenomas: Improved, Hormone WNL 5 (55.0%). Improved, Hormone still high 3 (32.5%) No hormonal improvement 1 (12.5%) |
| Acromegaly; Increased Growth hormone,GH-adenomas 6 (8.9%) | Acromegaly (GH adenomas) Improved, WNL 3 (43%). Improved, Hormone still high 4 (57%) | |
| Increased level of FSH1 (1.5) | ||
| Normal level of Prolactin 25 (37.3%) |
LH: Leutinizing hormone, GH: Growth hormone, FSH: Follicle stimulating hormone, WNL: Within normal limits, Pre-op: preoperatively, Post-op: postoperatively, %: percentage.
A Complete tumor excision could be achieved in 50 patients (74.6%) with no relapse. In 5 patients (7.4%), tumor could be partially excised due to large size and/ or poor accessibility. In 12 patients (17.9%) who had complete initial excision, recurrence occurred after variable time period ranging from 1 – 7 years. All underwent successful revised excision.
In addition, the correlation of the rate of the recurrent tumors operatedvia the TNTS approach was statistically significant as well: Pearson correlation 0.827, P-value = 0,022.
Two patients (3.0%) required postoperative radiation. Both of these patients were cases of prolactinoma and there was a significant clinical improvement after radiation treatment.
Histopathology examination of the excised tissue reported predominantly pituitary adenoma in 59 cases (88.1%). There was one patient with empty sella syndrome (Table 1).
Rhinorrhea/CSF leakages were noted in 13 patients (19.4%). All of these patients responded to lumbar drainage for a variable period of 3 - 5 days. However, a dual strategy of lumbar drain combined with placement of fat at the leakage site was successfully adopted in 5 patients. 8 patients (11.9%) developed diabetes insipidus and polyuria. They responded to desmopressin. There was only 1 (1.5%) death in this series.
Discussion
There are two operative techniques for the resection of pituitary tumors. TSTN resection is the operative technique of choice; craniotomy being reserved for extra-sellar tumors only[6]. Surgical treatment is usually the first-line of treatment in pituitary adenomas - except for prolactinomas. In patients of prolactinomas, dopamine agonists are recommended as the preferred choice[6,7].
In the present series also, 13 of the 36 patients of prolactinomas (36.1%) had received either Bromocriptin or Cabergolinor Parlodelas the initial management strategy. In addition two patients each had received Thyroxine, Hydrocortisone and Testosterone. The advantage offered by surgical excision is the quick relief in sign and symptoms of the disease as well as prevention in the adverse effect of excessive hormone secretion on the target organs.
Last 5-7 years have seen emergence of stereotactic and fractional radiosurgery such as Gamma Knife or Cyber Knife as interventional treatment optionsfor single or combined management before or after surgical intervention[8]. However, results of large series with this treatment option and their follow-up are still awaited.
The incidence of secretory tumors in this series was 67.2%. Of these, 53.7% were noted to be actively secreting prolactin followed by growth hormone. This is in accordance to literature that reports 65% pituitary adenomasto be secreting an active hormone with 48% being prolactin[1].
Preoperative CT or MRI showed tumor size ranging between 5.7 X 5.7 mm to 49.5 X 35.5 mm in this series. Some of our tumor sizes were much bigger than that reported in other studies[4]. This could be due to late reporting to Hospital by patients largely out of ignorance.
The incidence of recurrence in this series was noted to be 17.9% (12 patients). 10 of thesepatients were re-operated successfully via TSTN route. However, 2 patients underwent craniotomy to excise their recurrence. The recurrence incidence of 17.9% in this series was significantly less than that reported from a study conducted in France and Belgium with a recurrence range of 24 - 61%[4]. This could be attributed to the routine use of neuronavigation and operating microscope by our operating unit.Our results are closer to the 15.04% recurrence reported by Roelfsema, Biermasz & Pereira in 2012[5]. Like in earlier studies[5,9], the present series also noted a higher incidence of recurrence in patients with prolactinomas.
Of the recurrent tumors, 11 belonged to the invasive grade IV and asymmetrical (subtype D: 7; subtype E: 4) One single case of grade IV was symmetrical (subtype B). (See Figure 1 below). In these cases, the TNTS did not approach these tumors ideally.
In the present series, we noted that all patients were operated using neuronavigation and operating microscope with a complete improvement in patient’s signs and symptoms in 68.9% after the first operation. (Tables 3 and 4).
Hardy’s classification of pituitary adenomas. Grades I and II are enclosed within the sella. Grades III and IV are invasive. Extrasellar classifications A, B, and C are increasing amounts of direct suprasellar adenomas. D is asymmetric extension, and E is lateral extension into the cavernous sinus. (Adapted from Hardy J, Somma M. 1979).
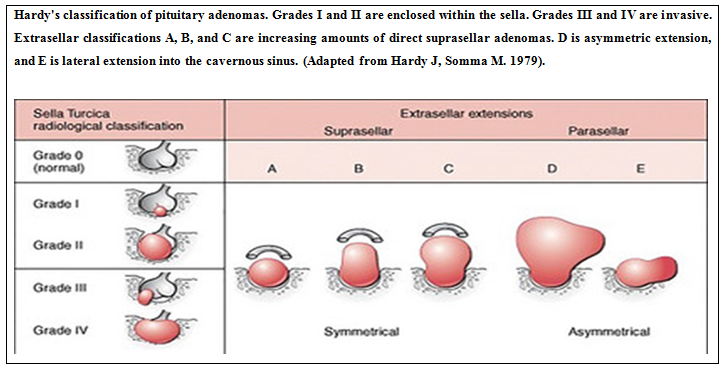
Table 3: Clinical improvement of the symptoms of patients as relationship / comparison between the pre- and postoperative period.
| Preoperatively | Postoperatively |
|---|---|
| (Number of patients, (%)) | (Number of patients, (%)) |
| Headache 56 (83.6) | 12 (17.0) |
| Visual disturbance 28 (41.8) | 11 (16.4) |
| Cushing’s 10 (14.9) | 6 (8.9) |
| Menstrual disturbance 9 (13.4) | 5 (7.4) |
| Hypertension 5 (7.5) | 3 (4.4) |
| Loss of libido 4 (6.0) | 2 (3) |
| Dyslipidemia 3 (4.5) | 2 (3) |
| Lactorrhea 3 (4.5) | 1 (1.5) |
| Psychotic problems 1 (1.5) | 0 |
| Nausea 1 (1.5) | 0 |
| Tinnitus 1 (1.5) | 0 |
| Large breast 1 (1.5) | 1 (1.5) |
| Facial palsy 1 (1.5) | 1 (1.5) |
| Proptosis 1 (1.5) | 1 (1.5) |
| Bitemporal hemianopia 1 (1.5) | 0 |
Table 4: Endocrine medication of the patientsin the pre- and postoperative period.
| Preoperatively | Postoperatively |
|---|---|
| Bromocriptin (6) | 3 |
| Cabergolin (5) | 2 |
| Parlodel (2) | 1 |
However, 16 patients (23.9%) had to undergo a revision surgery for complete relief of their symptoms. There were only 4 patients (5.9%) who showed no improvement in their symptoms.
Intraoperative MRI facility does not exist at our center. However, it may be noted that intraoperative MRI scans may be useful in some patients but are not generally recommended[10,11].
Pituitary tumors are reported to occur more frequently in women than in men, particularly between the second and third decades of life, when the ratio is estimated to be 10:1. After the fifth decade of life, the frequency of prolactinomas is similar in both sexes[12]. In this series, the overall incidence of female to male ratio was 43:24 establishing a female preponderance. However, others have reported an identical incidence in either sex[1].
The single death is this series was a patient with high level of growth hormone, but low level of testosterone with headache, behavioral changes and acromegaly. He was noted to be in poor general condition. The patient suffered middle cerebral artery spasm that could not be relieved. After 3 days the patient deteriorated and underwent craniectomy. He continued to deteriorate and died 3 days later.
An interesting finding in this retrospective analysis has been a relatively high incidence of pituitary tumor apoplexy in 17 patients (25.4%) as seen by preoperative CT and or MRI. This constitutes a medical emergency due to acute infarction or hemorrhage in the pituitary gland. In majority of patients it happens without any predisposing factors[13]. Some known predisposing factors include therapy with Bromocriptine and Cabergoline[14].
Trans-sphenoidal excision is the procedure of choice in patients with apoplexy especially those with bleeding pituitary adenomas[13].
Conclusion
The incidence of functioning pituitary adenomas was 67.2% with an overall recurrence rate of 17.9%, whereas the tumors belonged to the invasive and mostly the asymmetrical tumor subtypes retrospectively.
This retrospective analysis indicates that headache was, among other symptoms, the commonest presenting symptom (83.6%) in this study. These symptoms have improved significantly after surgery.
A significant rate of clinical improvement of the patients was recorded after the first surgical intervention.
The most important complication was a CSF leak (19.4%), which was fully cured in all patients by using a lumbar drainage catheter and / or placement of fat at the leakage site.
References
1. Greenberg, M.S. Pituitary tumors-general information and classification In Handbook of neurosurgery. 8th Ed. (2016) Thieme Medical Publishers, Inc: New York 719-729.
PubMed||CrossRef||Others
2. Ezzat, S., Asa, S.L., Couldwell, W.T., et al. The prevalence of pituitary adenomas: a systematic review. (2004) Cancer 101(3): 613–619.
3. Arafah, B.M., Nasrallah, M.P. Pituitary tumors: pathophysiology, clinical manifestations and management. (2001) Endocr Relat Cancer 8(4): 287–305.
4. Brochier, S., Galland, F., Kujas, M., et al. Factors predicting relapse of nonfunctioning pituitary macroadenomas after neurosurgery: a study of 142 patients. (2010) Eur J Endocrinol 163(2): 193-200.
5. Roelfsema, F., Biermasz, N.R., Pereira, A.M. Clinical factors involved in the recurrence of pituitary adenomas after surgical remission: a structured review and meta-analysis. (2012) Pituitary 15(1): 71-83.
6. Colao, A., Savastano, S. Medical treatment of prolactinomas. (2011) Nat Rev Endocrinol 7(5): 267–278.
7. Biller, B.M.K., Grossman, A.B., Stewart, P.M., et al. Treatment of adrenocorticotropin-dependent Cushing’s syndrome: a consensus statement. (2008) J Clin Endocrinol Metab 93(7): 2454–6242.
8. Winder, M.J., Mayberg, M.R. Recent advances in pituitary tumor management. (2011) Curr Opin Endocrinol Diabetes Obes 18(4): 278–288.
9. Symon, L., Logue, V., Mohanty, S. Recurrence of pituitary adenomas after Transcranial operation. (1982) J Neurol Neurosurg Psychiatry 45(9): 780-785.
PubMed||CrossRef||Others
10. Buchfelder, M., Schlaffer, S. Intraoperative magnetic resonance imaging during surgery for pituitary adenomas: pros and cons. (2012) Endocrine 42(3): 483–495.
11. Mehta, G.U., Jane, J.A Jr. Pituitarytumors. (2012) Curr Opin Neurol 25(6): 751–755.
12. Mindermann, T., Wilson, C.B. Age-related and gender-related occurrence of pituitary tumors. (1994) Clin Endocrinol 41(3): 359–3 64.
13. Chang, C.V., Felicio, A.C., Toscanini, A.C. Pituitary tumor apolplexy. (2009) Arq Neuropsiquitar 67(2A): 328-333.
14. Vella, A., Young, Jr. W.F. Pituitary apoplexy. (2001) Endocrinologist 11(4): 282-288.
PubMed||CrossRef||Others










