
Association between the Urokinase Plasminogen Activation System Polymorphisms and NSCLC in Chinese Population
Jianzhong Gu1, Yingying Shen1, Yongjun Zhang2*
Affiliation
- 1The First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, China
- 2Department of Integration of Traditional Chinese and Western Medicine, Zhejiang Cancer Hospital, Hangzhou, China
Corresponding Author
Yongjun Zhang, Department of Integration of Traditional Chinese and Western Medicine, Zhejiang Cancer Hospital, 38 Banshan Road, Hangzhou 310022, China, E-mail: zhangyj@zjcc.org.cn
Citation
Zhang, Y., et al. Association between the Urokinase Plasminogen Activation System Polymorphisms and NSCLC in Chinese Population. (2016) Int J Cancer Oncol 3(3): 1- 6.
Copy rights
© 2016 Zhang, Y. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Chinese population; Non-small cell lung cancer; uPA; uPAR; Polymorphism
Abstract
Aim: To evaluate the influence of uPA and uPAR gene polymorphisms in the susceptibility to NSCLC.
Methods: A total of 500 NSCLC patients and 500 healthy controls were recruited and matched according to age and gender. The SNPs distributed in uPA and uPAR gene were selected for genotyping. The association between genotype and NSCLC risk was evaluated by computing the OR and 95% CI with multivariate unconditional logistic regression analyses.
Results: Patients with the uPAR rs344781 T allele had a reduced risk of developing SCC patients (OR = 0.742; 95% CI = 0.579 - 0.950; P = 0.0176), especially a risk of developing male SCC patients (OR = 0.722; 95% CI = 0.546 - 0.954; P = 0.0219). And the uPAR rs344781 C/C allele homozygote was associated with an increased risk of SCC in patients (OR = 1.713; 95% CI = 1.145 - 2.563; P = 0.0083). However, neither allele frequencies nor genotype frequencies in uPA rs4065 were associated with NSCLC (P > 0.05).
Conclusions: Our results revealed that genetic polymorphisms of uPAR rs344781 were associated with the risk of developing SCC (squamous cell carcinoma) in a Chinese population.
Introduction
Extracellular Matrix (ECM) degradation mediated by the urokinase plasminogen activation (uPA) system is an important mechanism involved in both physiological and pathological tissue remodeling[1,2]. Many experimental and clinical studies have demonstrated the association of uPA system activity with cancer invasion and metastasis, including lung cancer[3,4]. Members of uPA system, including uPA and its receptor (uPAR), play critical roles in proteolysis, migration, invasion, and metastasis[5,6]. The median levels of uPA and uPAR expression are higher in lung tumor tissues than the adjacent lung parenchyma.
Lung cancer is the leading cause of cancer death around the world, due to its high mortality and morbidity[7]. In China alone, the incidence and mortality associated with lung cancer are estimated to be 0.7 and 0.6 million cases, respectively[8]. Pathologically, genetic and environmental interactions play a key role in the development and progression of lung cancer[9]. However, these interactions are dependent on genetic variations or single nucleotide polymorphisms (SNPs). Recently, one study in Taiwan has shown that genetic polymorphisms of the uPA rs4065 C/T and uPAR rs344781 (-516 T/C) were associated with the susceptibility and severity of NSCLC[10]. Although Taiwan and the Chinese mainland are similar in some ways, their living environment and diet were in different ways. In this study, the relationship between SNPs of uPA, uPAR, and NSCLC risk on the Chinese mainland were investigated, and the impact of these SNPs on susceptibility and clinicopathological characteristics of NSCLC were also evaluated.
Materials and Methods
Study population
In this study, we recruited 500 NSCLC patients and 500 unrelated age-matched healthy controls from The Zhejiang Cancer Hospital, Hangzhou, China between March, 2011 and April, 2012. All cases and controls were Chinese Han origin and lived in Zhejiang Province, China. Participants had no history of previous primary cancer other than lung cancer. The controls were independent lung-related diseases to avoid any probable interference from overlapping genes. Current smoker or former smoker or non-smokers were included. All subjects provided their informed consent approved by the Ethic Committee of Zhejiang Cancer Hospital.
SNPs selection and genotyping
uPA rs4065 and uPAR rs344781 were selected according to a previous study[11]. DNA was extracted from whole blood by AxyPrep Blood Genomic DNA Miniprep Kit (Axygen Biosciences, Union City, CA). The uPA SNP and uPAR SNP of interest were then genotyped using the SEQUENOM Mass ARRAY matrix-assisted laser desorption ionization-time of flight mass spectrometry platform (Sequenom, San Diego, CA). PCR primers and single base extension primers were designed using Assay Designer’s software version 3.0 (Sequenom) and synthesized by Sangon Biotech (Shanghai, China). The sequences of forward and reverse primers were as follows: 5′-ACGTTGGATGAAGAGACTGGGAAGATAGGC- 3′ and 5′-ACGTTGGATGGCCTGAGGGTAAAGCTATTG- 3′ for uPA rs4065 (104 bps); 5′-ACGTTGGATGCACATTCCTTTAACATTTACC-3′ and 5′-ACGTTGGATGAACACTTAACCCTTGCTTT-3′ for uPAR rs344781 (115 bps).
Statistical analysis
All statistical analyses were performed using SPSS 13.0 for Windows (SPSS Inc., Chicago, IL). Hardy-Weinberg equilibrium (HWE) was carried out for all SNPs, cases and controls were compared using the χ² test with a P-value of < 0.001 being considered statistically significant. The χ² test was used to assess the frequencies of the selected allele and genotype between the cases and controls. The association between SNPs and NSCLC risk was analyzed by computing the odds ratio (OR) and 95% confidence interval (CI) from multivariate unconditional logistic regression analysis. A two-sided P < 0.05 was considered statistically significant.
Results
500 patients (350 males and 150 females) and 500 healthy controls (259 males and 240 females, and gender information for one control subject was missed) were of Chinese Han origin. For NSCLC patients, 331 had adenocarcinoma (ADC), and 169 had squamous-cell carcinomas (SCC); 280 male and 21 female patients were smokers or former smokers, while 189 male and 14 female of the controls were smokers or former smokers. The studied population were within HWE (P = 0.17109 for uPA rs4065; P = 0.14444 for uPAR rs344781, respectively).
The allele frequency of uPA rs4065 was 12.6% (T) and 87.4% (C) in NSCLC patients, 12.7% (T) and 87.3% (C) in ADC patients, 12.4% (T) and 87.6% (C) in SCC patients, and 12.5% (T) and 87.5% (C) in controls. No statistical differences in allele frequencies of these four SNPs were found between the case and control subjects (P > 0.05). Stratification by gender revealed no significant difference in allele frequencies (P > 0.05). (Table 1,2,3). Allele frequency of uPAR rs344781 was 51.8% (T) and 48.2% (C) in NSCLC patients, 54.2% (T) and 45.8% (C) in ADC patients, 47.0% (T) and 53.0% (C) in SCC patients, and 54.5% (T) and 45.5% (C) in controls. In patients with SCC, the allele frequencies in uPAR rs344781 were significantly different from the controls (OR = 0.742; 95% CI = 0.579 - 0.950; P = 0.0176). We then stratified by analysis of gender, the allele frequencies in uPAR rs344781 were significantly different between male SCC patients and male controls (OR = 0.722; 95% CI = 0.546 - 0.954; P = 0.0219). The T allele was found to be associated with a lower risk for SCC development, and it may be a potential lower-risk marker for male SCC patients in China. (Table 1,2,3).
Table 1: Allele frequency of uPA and uPAR SNPs in NSCLC patients and healthy controls.
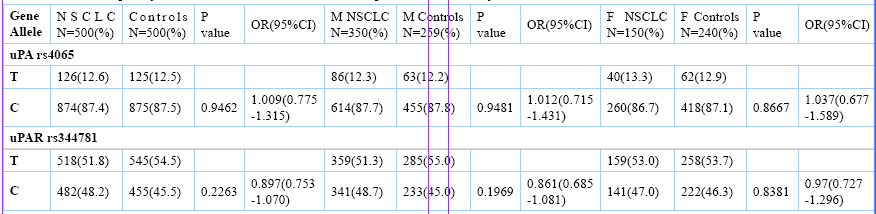
NSCLC, Non-small cell lung cancer; M, Male; F, Female.
Table 2: Allele frequency of uPA and uPAR SNPs in ADC patients and controls.
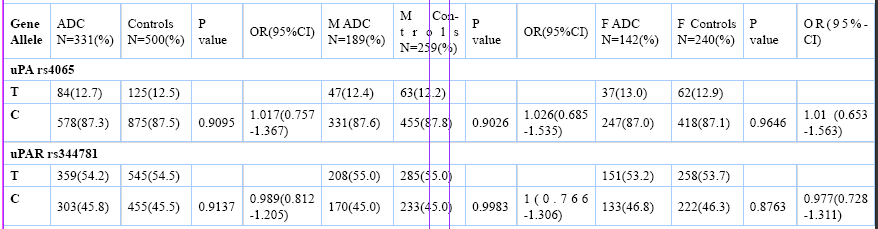
ADC, adenocarcinoma; M, Male; F, Female.
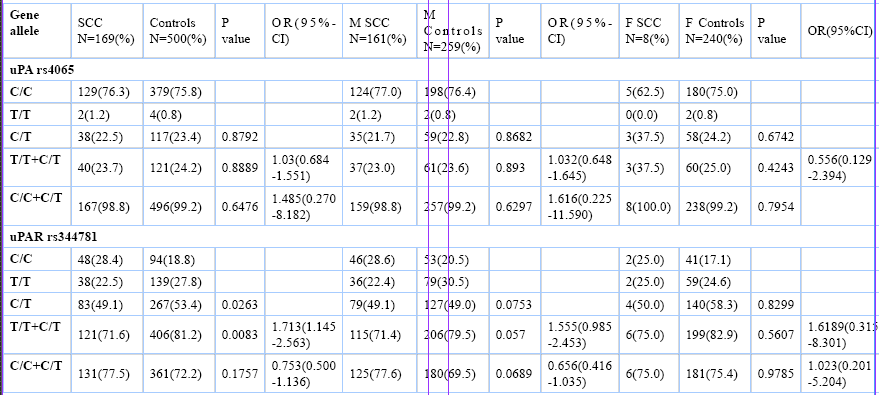
Table 3: Allele frequency of uPA and uPAR SNPs in SCC patients and controls.

SCC, squamous cell carcinoma; M, Male; F, Female.
Genotype frequencies of uPA rs4065 genotype were 76.2% (C/C), 1.4% (T/T) and 22.4% (C/T) in NSCLC patients, 76.1% (C/C), 1.5% (T/T) and 22.4% (C/T) in ADC patients, 76.3% (C/C), 1.2% (T/T) and 22.5% (C/T) in SCC patients, 75.8% (C/C), 0.8% (T/T), and 23.4% (C/T) in the controls. No statistical differences in allele frequencies of these four SNPs were found between the case and control subjects (P > 0.05). Stratification by gender revealed no significant difference in genotype frequencies (P > 0.05). Genotype frequencies of uPAR rs344781 were 22.8% (C/C), 26.4% (T/T) and 50.8% (C/T) in NSCLC patients, 19.9% (C/C), 28.4% (T/T) and 51.7% (C/T) in ADC patients, 28.4% (C/C), 22.5% (T/T) and 49.1% (C/T) in SCC patients, 18.8% (C/C), 27.8% (T/T), and 53.4% (C/T) in the controls. There were statistically significant differences for the C/C, T/T, and C/T genotypes between SCC patients and controls (P = 0.0263). When analyzing the association between genotypes and the risk of SCC, logistic regression analysis revealed that the uPAR rs344781 C/C allele homozygote was associated with an increased risk of SCC in patients (OR = 1.713; 95% CI = 1.145 - 2.563; P = 0.0083). (Table 4,5,6).
Table 4: Genotypes of uPA and uPAR SNPs in NSCLC patients and controls.
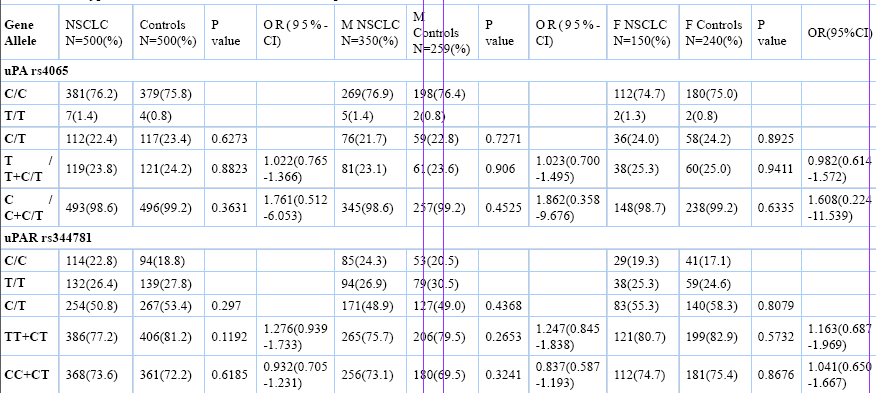
NSCLC, Non-small cell lung cancer; M, Male; F, Female.
Table 5: Genotypes of uPA and uPAR SNPs in ADC patients and controls.
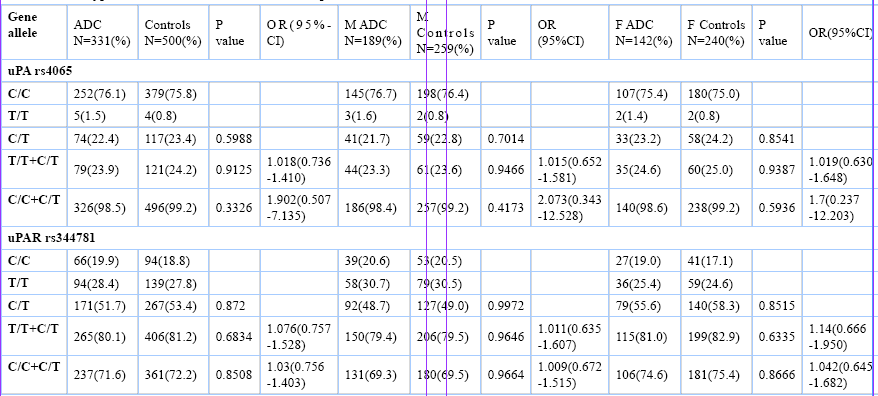
ADC, adenocarcinoma; M, Male; F, Female.
Table 6: Genotypes of uPA and uPAR SNPs in SCC patients and controls.
SCC, squamous cell carcinoma; M, Male; F, Female.
Discussion
In the current study, we investigated the association between SNPs (uPA rs4065 and uPAR rs344781) and the risk of developing NSCLC. Indeed, we found that patients with the uPAR rs344781 T allele had a reduced risk of developing SCC patients, especially a reduced risk of developing male SCC patients. And the uPAR rs344781 C/C allele homozygote was associated with an increased risk of SCC in patients. However, neither allele frequencies nor genotype frequencies in uPA rs4065 were associated with NSCLC.
Tumor invasion and metastasis require proteolytic enzymes that destroy the extracellular matrix and enhance the formation of novel blood vessels[11]. The uPA system is thought to play a role in several different processes important to tumor progression including tissue remodeling, chemotaxis, tumor invasion, dissemination, proliferation, and angiogenesis[12,13]. The binding of uPA to uPAR increases the efficiency of plasminogen activation and also serves to localize these proteolytic cascades to the migrating or invading edge of cells[5,14,15]. Binding of uPA and vitronectin also promotes cell adhesion and cell migration. In addition, uPAR also interacts with various cell surface receptors such as integrins, growth factor receptors and endocytic receptor 180[16-18]. These interactions activate diverse signaling pathways including FAK, Src, MAPK and PI3K, leading to EMT, cell proliferation, cell migration and the expression of pro-cancer genes[5,19,20]. These signaling pathways play important roles in NSCLC[21-24]. In accordance with these studies, our study indicated uPAR maybe susceptibility gene involved in NSCLC development. In this study, the uPAR rs344781 polymorphism was inversely associated with the development of lung SCC in a Chinese population. C/C homozygote individuals had a 1.713-fold increased risk in developing NSCLC compared to T/T homozygote or C/T heterozygote individuals. In addition we found that T allele had a 0.742-fold reduced risk of developing SCC patients, and a 0.722-fold reduced risk of developing male SCC patients.
Lung cancer is a complex disease resulting from environmental factors, genetic factors, and their interactions[25,26]. The possibility that the relationship between the uPA/uPAR genotypes with NSCLC susceptibility in the study is an ethnic-dependent observation cannot be entirely excluded because multiple risk factors and etiology contribute to the pathophysiology of NSCLC development. Our results are not in agreement with those found in a study by Chuen-Ming Shih[10]. Together with earlier studies[27-29], these differences may primarily be attributed to the different living environments.
Conclusion
In conclusion, our results revealed that genetic polymorphisms of uPAR rs344781 were associated with the susceptibility NSCLC. The results of this study uncover the significant relationship between genetic polymorphisms of uPAR with the susceptibility of NSCLC. However, there are three limitaions in our study. First, the small sample size may be a limitation of the present study. Second, we found that uPAR rs344781 polymorphisms were associated with the development of SCC in a Chinese population, would be better illustrated the effect of uPAR rs344781 polymorphisms in SCC cell proliferation if we preformed functional studies of uPAR rs344781 polymorphisms in vitro. Third, population stratification may have led to a bias.
Acknowledge:
This study was supported in part by grants from Zhejiang Provincial Natural Science fund (#LY13H290006).
Conflict of interest:
None declared.
Author’s contributions:
Yongjun Zhang and Jianzhong Gu designed this study, performed the statistical analysis, and drafted the manuscript. Yingying Shen carried out the collection of samples and helped to draft the manuscript.
References
- 1. Madsen, C.D., Sidenius, N. The interaction between urokinase receptor and vitronectin in cell adhesion and signalling. (2008) Eur J Cell Biol 87(8-9): 617-629.
- 2. Xu, S., Grande-Allen, K.J. The role of cell biology and leaflet remodeling in the progression of heart valve disease. (2010) Methodist Debakey Cardiovasc J 6: 2-7.
- 3. Gutova, M., Najbauer, J., Frank, R.T., et al. Urokinase plasminogen activator and urokinase plasminogen activator receptor mediate human stem cell tropism to malignant solid tumors. (2008) Stem Cells 26(6): 1406-1413.
- 4. Carriero, M.V., Longanesi-Cattani, I., Bifulco, K., et al. Structure-based design of an urokinase-type plasminogen activator receptor-derived peptide inhibiting cell migration and lung metastasis. (2009) Mol Cancer Ther 8(9): 2708-2717.
- 5. Noh, H., Hong, S., Huang, S. Role of urokinase receptor in tumor progression and development. (2013) Theranostics 3(7): 487-495.
- 6. Shariat, S.F., Roehrborn, C.G., Mc Connell, J.D., et al. Association of the circulating levels of the urokinase system of plasminogen activation with the presence of prostate cancer and invasion, progression and metastasis. (2007) J Clin Oncol 25(4): 349-355.
- 7. Edwards, B.K., Noone, A.M., Mariotto, A.B., et al. Annual Report to the Nation on the status of cancer, 1975-2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. (2014) Cancer 120(9): 1290-1314.
- 8. He Jie, Chen Wanqing. Chinese cancer registry annual report (2012) Beijin, China; Military medicine society press.
- 9. Matakidou, A., Eisen, T., Houlston, R.S. Systematic review of the relationship between family history and lung cancer risk. (2005) Br J Cancer 93(7): 825-833.
- 10. Shih, C.M., Kuo, W.H., Lin, C.W., et al. Association of polymorphisms in the genes of the urokinase plasminogen activation system with susceptibility to and severity of non-small cell lung cancer. (2011) Clinica Chimica Acta 412(1-2): 194-198.
- 11. Tsai, J.P., Hsiao, P.C., Yang, S.F., et al. A suppresses migration and invasion of human hepatocellular carcinoma cells through down regulation of MKK4/JNK via NF-κB mediated urokinase plasminogen activator expression. (2014) PLoS One 9: e86537.
- 12. Weidle, U.H., Konig, B. Urokinase receptor antagonists: novel agents for the treatment of cancer. (1998) Expert Opin Investig Drugs 7(3): 391-403.
- 13. Lakka, S.S., Rajagopal, R., Rajan, M.K.,et al. Adenovirus-mediated antisense urokinase-type plasminogen activator receptor gene transfer reduces tumor cell invasion and metastasis in non-small cell lung cancer cell lines. (2001) Clin Cancer Res 7(4):1087-1093.
- 14. Mekkawy, A.H., Morris, D.L., Pourgholami, M.H. Urokinase plasminogen activator system as a potential target for cancer therapy. (2009) Future Oncol 5(9): 1487-1499.
- 15. Waltz, D.A., Natkin, L.R., Fujita, R.M., et al. Plasmin and plasminogen activator inhibitor type 1 promote cellular motility by regulating the interaction between the urokinase receptor and vitronectin. (1997) J Clin Invest 100(1): 58-67.
- 16. Tang, C.H., Hill, M.L., Brumwell, A.N., et al. Signaling through urokinase and urokinase receptor in lung cancer cells requires interactions with beta1 integrins. (2008) J Cell Sci 121: 3747-3756.
- 17. Engelholm, L.H., Nielsen, B.S., Dano, K., et al. The urokinase receptor associated protein (uPARAP/endo180): a novel internalization receptor connected to the plasminogen activation system. (2001) Trends Cardiovasc Med 11(1): 7-13.
- 18. Bass, R., Werner, F., Odintsova, E., et al. Regulation of urokinase receptor proteolytic function by the tetraspanin CD82. (2005) J Biol Chem 280(15): 14811-14818.
- 19. Alfano, D., Franco, P., Vocca, I., et al. The urokinase plasminogen activator and its receptor: role in cell growth and apoptosis. (2005) Thromb Haemost 93(2): 205-211.
- 20. Blasi, F., Carmeliet, P. uPAR: a versatile signalling orchestrator. (2002) Nat Rev Mol Cell Biol 3(12): 932-943.
- 21. Kitano, H., Chung, J.Y., Ylaya, K., et al. Profiling of phospho-AKT, phospho-mTOR, phospho-MAPK and EGFR in non-small cell lung cancer. (2014) J Histochem Cytochem 62(5): 335-346.
- 22. Shieh, J.M., Cheng, T.H., Shi, M.D., et al. α-Tomatine suppresses invasion and migration of human non-small cell lung cancer NCI-H460 cells through inactivating FAK/PI3K/Akt signaling pathway and reducing binding activity of NF-κB. (2011) Cell Biochem Biophys 60(3): 297-310.
- 23. Wilson, C., Nicholes, K., Bustos, D., et al. Overcoming EMT-associated resistance to anti-cancer drugs via Src/FAK pathway inhibition. (2014) Oncotarget 5(17): 7328-7341.
- 24. Papadimitrakopoulou V. Development of PI3K/AKT/mTOR pathway inhibitors and their application in personalized therapy for non-small-cell lung cancer. (2012) J Thorac Oncol 7(8): 1315-1326.
- 25. Hoover, R.N. Cancer-nature, nurture, or both. (2000) N Engl J Med 343(2): 135-136.
- 26. Zhang, R., Chu, M., Zhao, Y., et al. A genome-wide gene-environment interaction analysis for tobacco smoke and lung cancer susceptibility. (2014) Carcinogenesis 35(7): 1528-1535.
- 27. Zhang, Y., Shi, H., Zhang, A., et al. Association between polymorphisms in COMT, PLCH1, and CYP17A1, and non-small-cell lung cancer risk in Chinese nonsmokers. (2013) Clin Lung Cancer 14(1): 45-49.
- 28. Zhang, Y., Gu, C., Shi, H., et al. Association between C3orf21, TP63 polymorphisms and environment and NSCLC in never-smoking Chinese population. (2012) Gene 497(1): 93-97.
- 29. Kueh, K.S., Loffredo, C.A. Genetic and environmental influences on malformations of the cardiac outflow tract. (2005) Expert Rev Cardiovasc Ther 3(6): 1125-1130.










