
CAD/CAM Technology and Fabrication of Ceramic Inlay for an Endodontically Treated Tooth
Abdul Hameed Nader, O’Neill Ed, Howard Stephen
Affiliation
- College of Dentistry, Department of Restorative Dental Science, Prosthodontics Division, University of Florida, Gainesville, USA
Corresponding Author
Castellanos E. Mauricio, College of Dentistry, Department of Restorative Dental Science, Prosthodontics Division, University of Florida, Gainesville, USA. Tel: 919-360-1531; E-mail: ecastellanos@dental.ufl.edu
Citation
Castellanos, E. M., et al. CAD/CAM Technology and Fabrication of Ceramic Inlay for an Endodontically Treated Tooth. (2015) J Dent & Oral Care 1(2): 1- 3.
Copy rights
©2015 Castellanos, E. M. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Inlays; CAD/CAM; Lithium Disilicate
Abstract
The improvement of digital dentistry such as the intraoral scanners and all-ceramics restorations that can be fabricated with computer-assisted design/ computer-assisted manufacturing (CAD/CAM) technology, have changed clinicians approach for treating patients. This case report describes the fabrication of lithium disilicate inlay on an endodontically treated mandibular second molar with CAD/CAM restoration offering aconservative alternative for patients. Purpose: The purpose of this article is to provide information on a particular technique to manage a case of an endodontically treated tooth by performing a treatment combining digital dentistry with conventional lab work. This technique will demonstrate efficient the fabrication and adjustmentof lithiumdisilicate inlay restoration.
Introduction
The combination of advancements in dental materials as well as in computer technology has made CAD/CAM-fabricated restorations possible and plentiful in dental clinics. As a result, all-ceramic restorations have become both a necessary alternative to metal–ceramic systems, as well as a preferred choice for some clinicians due to patient's esthetic request. These new all-ceramic systems can use a monolithic glass–ceramic material. IPS e.max (Ivoclar Vivadent) is one of the most popular system in the market. An example of a chair side system is the computer-assisted Ceramic Reconstruction System (CEREC®, Sirona Dental Systems), which was the first operational CAD/CAM system to be used in the dental office[1].
The CAD/CAM systems that are used in dental applications generally consist of three modules[2]. The first module is a scanner, which scans a solid model and intraoral scan can be done and converts the model into digital data. The second module is a design software package, which is used to design and modify the digital model; and finally a milling machine, which mills the designed model using a selected material[3-4]. Another example of a chair side system is the Planmeca-E4D Technologies LLC, which uses an intraoral digitizer laser, which requires no powder to capture the prepared teeth.
Ceramic systems have utilized single-layer techniques (monolithic) such as feldspathic ceramic or leucite-reinforced glass-ceramics. A lithium disilicate restorative material (IPS e. max CAD), which was initially designed for use in double-layer techniques such as a coping material, is now available in different shades and different translucencies for use in esthetic full-contour single-layer (monolithic) restorations[5,6]. Partial crystallization enables fast machining with CAD/ CAM systems (blue, translucent state). Following the milling procedure, the restorations are crystallized. In the course of this process, lithium disilicate crystals (Li2Si2O5) are formed, which impart the ceramic object with the desired high strength[7].
The E4D (D4D TECH) capture images using laser technology. This technology can be used for the fabrication of monolithic crowns chair side or in the laboratory with subsequent staining and characterization. Depending on the location of the components of the CAD/CAM systems the production can either be chair side, laboratory or centralized fabrication in a production center.
A prospective study comparing the 10-year outcome data of three-unit all-ceramic fixed dental prostheses (FDPs) fabricated from a monolithic lithium-disilicate ceramic (IPS e.max), in comparison with metal–ceramic FDPs reported the rate of ceramic chipping as 3% after 5 years and 6.1% after 10 years[7,8].
Case Report
Diagnosis and Treatment Planning
A 52 year old male with no contributory medical history, was referred to the graduate prosthodontic program at the University of Florida for replacement of provisional restoration of an endodontically treated tooth #31. Clinical findings showed patient with small amount of biofilm and the caries risk assessment was low, regarding tooth #31 was found more than 2 mm of intact enamel around access in the horizontal plane from the occlusal view. Also, patient had a resin-based composite restoration placed more than 10 years ago and failure was due to biological complications such as caries. Decision to not cover functional cusp was made taking into consideration preservation of more than 2 mm of enamel and occlusion which did not affect resin composite in more than 10 years.
Clinical Protocol
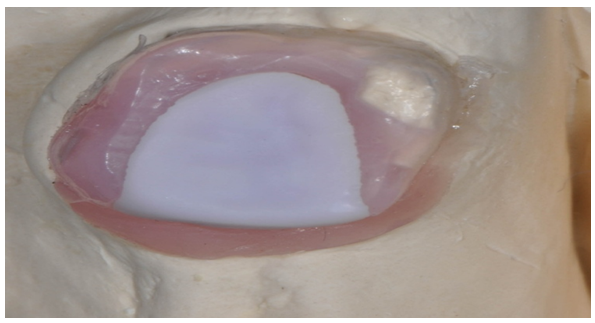
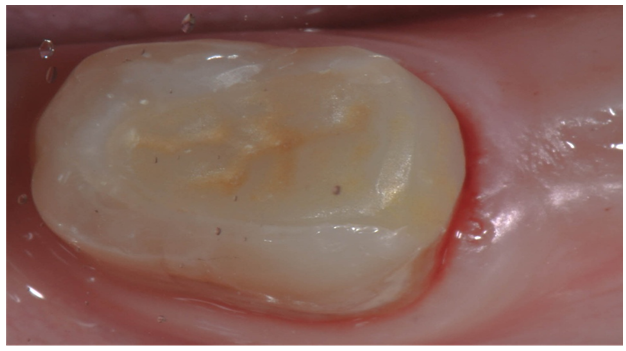
Preoperatively, occlusion was analyzed clinically, and then with the aid of mounted study cast on a semi-adjustable articulator (Denar 330, Lousville, KY). Provisional restoration was removed from tooth #31. Preparation for an inlay restoration was performed [Figure 1]. An impression was made with a disposable plastic tray and, heavy and wash body of a vinyl polysiloxane (VPS) matrix material Aquasil (Dentsply, NY). The impression was poured with Tissue Moulage Gingitech (Ivoclar, Vivadent) over the preparation, and a second pouring was made with gypsum product type III (WhipMix, Lousville, KY) [Figure 2]. This technique was applied in order to be able to place and remove restoration without causing damage of the ceramic or master cast. Intraoral scan of the preparation was obtained using the E4D/Planscan.

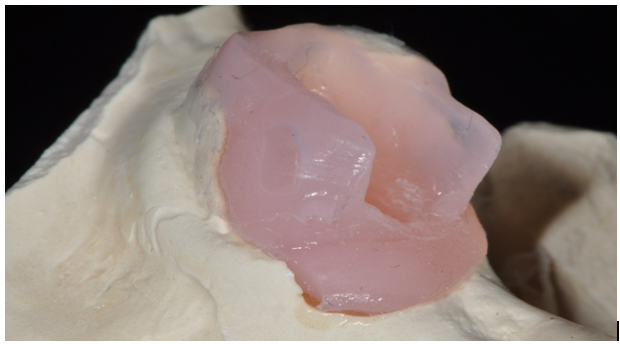
Figure 2: Tissue model of inlay preparation of tooth # 31. Combination of Gingitech and gypsum products
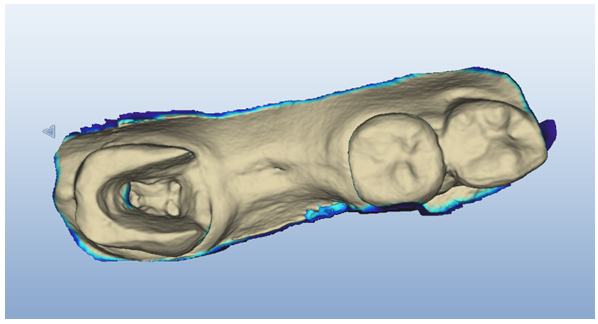
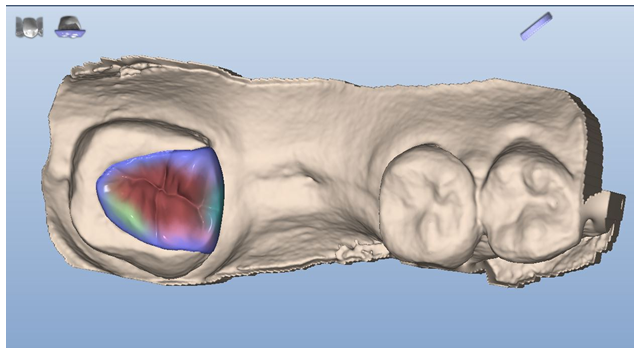
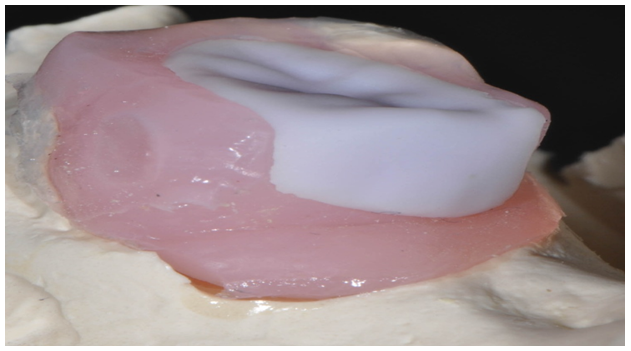
The E4D intraoral scanner was used for capturing image of tooth # 31 [Figure 3]. Restoration was designed following anatomic contour of tooth # 31 and occlusion was checked as well with the software [Figure 4]. IPS e.max CAD block was used with plameca milling machine. Restoration was milled in 21 minutes and placed in the blue state first on our tissue model cast [Figure 5,6]. Adjustments were made with a fine diamond stone following manufacture recommendations and restoration was placed intraorally in the blue state to confirm adjustment, margins and occlusion were inspected. Crystallization was performed in the Programat P500/G2 (Ivoclar, Vivadent) following manufacture's recommendations using an Ivoclar tray and object fix supporting all the restoration. Multilink (Ivoclar, Vivadent) was used for cementation following manufacture instructions [Figure 7].
Conclusion
While the basic fundamentals of tooth preparation still apply regardless of the method of restoration fabrication, the combination of new technology, digital impressions, and various materials that can be customized, milled and sintered, provide clinicians a more efficient chair side way to treat patients and provide all ceramic restorations in one appointment. Recent studies have shown CAD/CAM fabricated lithium disilicate restorations to be of high strength. This material is an excellent alternative to traditional restorations in a variety of clinical situations.
Some advantages of this technique are to avoid any chipping of the ceramic at the time of indirect adjustment in the cast. Also, reduce chair time at the time of delivery. Gingitech offers the properties to insert and remove the restoration without any chipping of the ceramic or the gypsum.
Combination of the new technology, keeping the basic fundamentals of tooth preparation regardless the restorations and milling different materials, provide clinicians a more efficient chair side effectiveness to treat patients in one appointment. CAD/CAM lithium silicate restorations provide high strength restorations that have been shown in recent studies.
References
- 1. Anderson, M., Razzoog, M. E., Oden, A., et al. Procera: a new way to achieve an all-ceramic crown. (1998) Quintessence Int 29(5): 285- 296.
- 2. Young, J. M., Altschuler, B. R. Laser holography in dentistry. (1977) J Prosthet Dent 38(2): 216- 225.
- 3. Estafan, D., Dussetschleger, F., Agosta, C., et al. Scanning electron microscope evaluation of CEREC II and CEREC III inlays. (2003) Gen Dent 51(5): 450- 454.
- 4. McLean, J. W. Perspectives of dental ceramics: proceedings of the First International Symposium on Ceramics. (1984) Quintessence 13- 40.
- 5. Bindl, A.,Mörmann, W. H. An up to 5-year clinical evaluation of posterior In-Ceram CAD/CAM core crowns. (2002) Int J Prosthodont 15(5): 451- 456.
- 6. Holmes, J. R., Bayne, S. C., Holland, G. A., et al. Considerations in measurement of marginal fit. (1989) J Prosthet Dent 62(4): 405- 408.
- 7. Barnfather, K. D., Brunton, P. A. Restoration of the upper dental arch using Lava all-ceramic crown and bridgework. (2007) Br Dent J 202(12): 731- 735.
- 8. IPS e.max Lithium Disilicate: The Future of All- Ceramic Dentistry. (2009) Ivoclar Vivadent 1- 14.










