
Clear Aligner Treatment with “In-Office” Virtual Model Set-Up and 3D Printing
Ling-Yu Chan1, Chung-Chen Jane Yao1,2, Yi-Jane Chen1,2*
Affiliation
- 1Division of Orthodontics and Dentofacial Orthopedics, Department of Dentistry, National Taiwan University Hospital, Taipei, Taiwan
- 2School of Dentistry, National Taiwan University, Taipei, Taiwan
Corresponding Author
Yi-Jane Chen, Division of Orthodontics and Dentofacial Orthopedics, Department of Dentistry, National Taiwan University Hospital, No. 1, Chang-Te Street, Taipei City, Taiwan, Tel: 886-2-23123456 ext 66863, Fax: 886-2-23831346; E-mail: lcyj@ntu.edu.tw
Citation
Chen, Y.J., et al. Clear Aligner Treatment with “In-Office” Virtual Model Set-Up and 3D Printing. (2017) J Dent Oral Care 3(2): 1- 5.
Copy rights
© 2017 Chen, Y.J. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Digital orthodontics; Clear aligner; Fused deposition modeling 3D printing
Abstract
Orthodontic treatment with clear aligners is increasingly popular in adult patients. Clear aligners can be applied more efficiently if virtual tooth movement set-ups and production of physical models did not require a third-party source. We here report digital orthodontic treatment with clear aligners to correct anterior tooth mal-alignment in a 28-year-old female patient. We scanned dental casts to create virtual models that we used to simulate orthodontic tooth movement. To create space to relieve crowding, we used arch expansion and interproximal re-approximation. Sequential virtual model set-ups were generated with the tooth movements programmed to be 0.3 ~ 0.4 mm in each step. We used an in-office 3D printer to produce physical models of virtual set-ups using polylactic acid material. Subsequently, we could fabricate clear aligners by use of physical models. At 3 and 7.5 months into treatment, we took dental impressions for mid-course correction due to off-tracking, i.e. predicted tooth movement not achieved as expected. After 11 months of treatment, alignment of the anterior teeth, incisor overjet and overbite had obviously improved. Meanwhile the occlusal contacts of the posterior teeth were maintained throughout the treatment period. The posttreatment occlusion improved significantly, both functionally and esthetically, and remained stable during the retention phase.
Introduction
Over the years, orthodontic treatments are becomingmore esthetic, comfortable, and easier to maintain in order to satisfy patients’ expectations. Because of its transparency, removable clear aligner therapy has become an increasingly popular alternative to fixed orthodontic appliances, and because it is less irritating and easier to brush and floss after meals. Kesling’s tooth positioner was the original model for clear aligners. Overlay appliances have achieved minor tooth movements using a technique developed by Ratintree Essix[1]. The Invisalign system, introduced in 1999 by Align Technology (Santa Clara, Calif), uses CAD-CAM stereolithography and tooth movement simulation software to move teeth incrementally with a series of clear aligners[2]. Nowadays, clear aligners have been applied in a wide range of treatments, even in orthognathic surgery cases[3]. Rossini et al. conducted a systematic review of the efficacy of clear aligners for orthodontic tooth movement[4]. The study summarized the research findings of two randomized clinical trials, as well as five prospective and four retrospective non-randomized studies. The amount of mean intrusion with aligners was 0.72 mm, and the movement accuracy was between 33% and 47%. Distal movement of upper molars showed the highest predictability (88%). Extrusion was the most difficult type of movement to achieve with aligners (30% of accuracy). In addition, a tooth with a short crown or a rounded shape is difficult to move with aligners. In extraction cases, treatment with aligners resulted in significant tipping of the teeth adjacent to extraction sites. Using composite attachments and appropriate auxiliaries, such as inter-arch elastics, can enhance tooth movement with aligners. Total treatment time using clear aligners may take longer than using fixed appliances alone[5]. Moreover, midcourse correction/refinement is often required to improve treatment effect[4,6].
With advances in scanning, CAD software, and rapid prototyping, clear aligner orthodontic treatment has become more widespread, leading in turn to the development of in-office digital orthodontics. As specialists, orthodontists have to play a critical role in determining tooth position and final occlusion. Fabricating physical models and clear aligners can save on cost and free orthodontists to adjust protocols based on patients’ clinical response, e.g. off-tracking, providing more efficient service delivery compared to outsourcing methods.
Case Report
The patient was a 28-year-old woman concerned about anterior teeth mal-alignment and asking for esthetic orthodontic treatment.
Diagnosis
The patient presented a straight profile with excessive gingival display on full smile. The upper dental midline deviated 2 mm to the left from her facial midline. Clinical examination showed Class I malocclusion with anterior teeth crowding¸ 4 mm overbite, and 3 mm over jet. Her upper left lateral incisor was lingually displaced showing cross-bite with the lower left lateral incisor (Figure1). Panoramic radiography did not show pathological findings (Figure 2). Cephalometric analysis revealed a Class I skeletal pattern with a hypo-divergent facial pattern.

Figure 1: Pre-treatment extra-oral and intra-oral photographs.
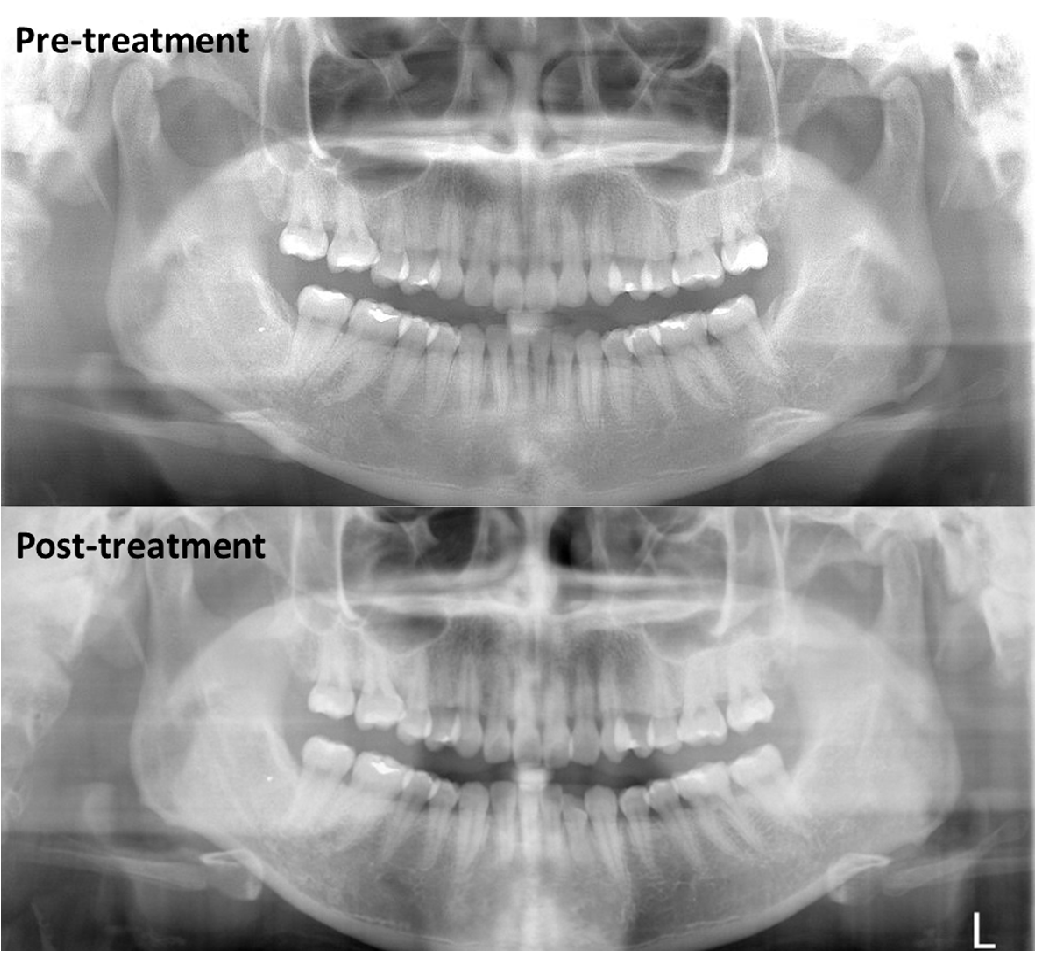
Figure 2: Pre-treatment and post-treatment lateral cephalograms.
Treatment objective and plan
The treatment aimed to improve the alignment and cross-bite of the anterior teeth without intervention for the posterior occlusion. The treatment with clear aligners was planned, and arch expansion as well as interproximal re-approximation (IPR) would create space to relieve the crowding.
Treatment progress
The treatment workflow was as follow. First, we used a non-contact laser scanner to scan the plaster models. The model images were then converted to a Standard Triangulation Language (STL) format. We used digital orthodontics software (3Shape®, Orthoanalyzer, Denmark) to plan and set up virtual models for orthodontic tooth movement. After the final occlusion was established, we generated sequential virtual models with tooth movements divided into 0.3 - 0.4 mm in each step. The physical models were then produced using Polylactic Acid (PLA) printing material and an in-office 3D printer (Ultimaker® 2+, Netherland) which applied a Fused Deposition Modeling (FDM) technique (Figure 3). Prior to printing, each virtual model in the STL format was tailored with the open-source software Meshmixer, then processed by the 3D printing slicing software Cura. The layer thickness was 0.1 mm and the average printing time was two hours per model. Aligners were made from transparent PET-G thermoplastic material (0.75 mm in thickness, Duran®, Scheu-Dental, Germany) using a printed physical model. The patient was instructed to wear the aligners full time, except when eating, drinking, or brushing teeth. Each aligner was to be worn basically two-weeks, but duration was occasionally extended due to patient factors.
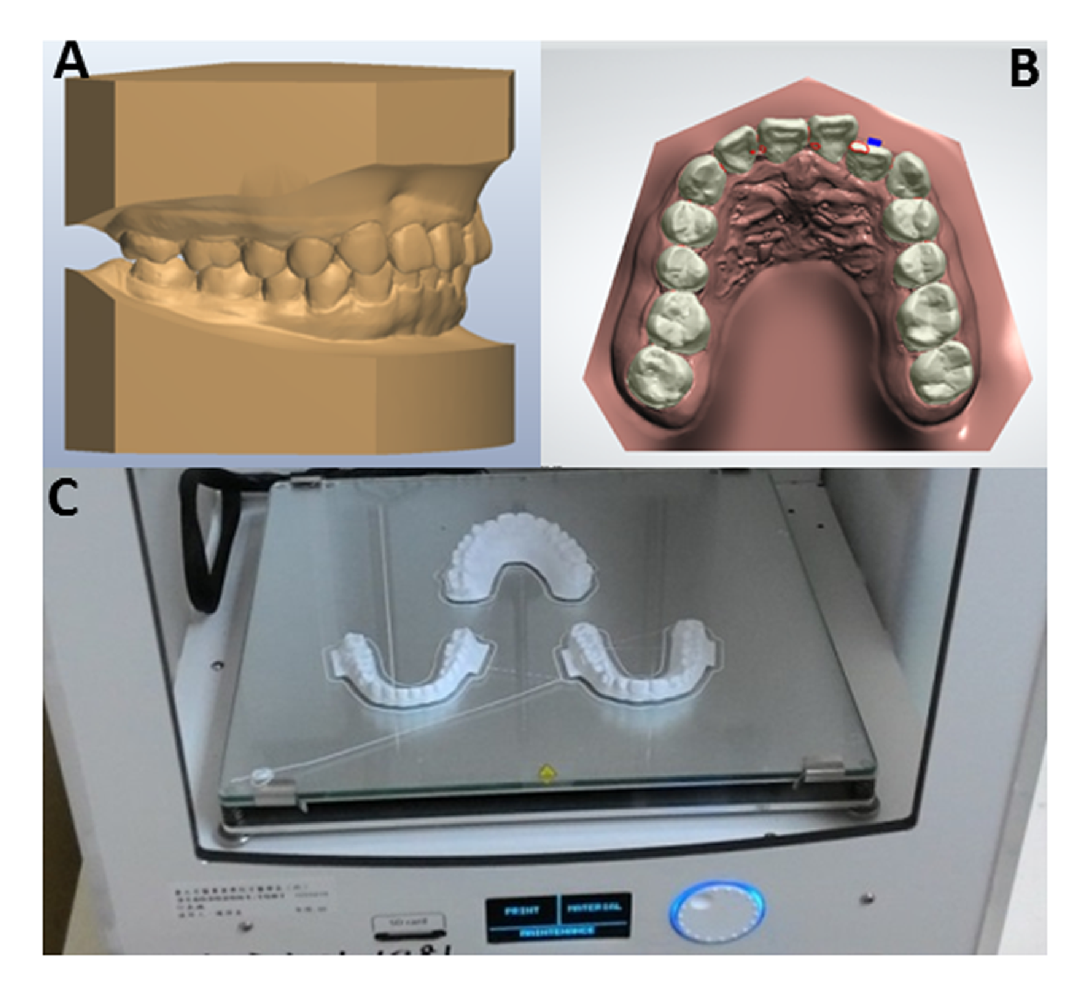
Figure 3: Preparation of physical models for fabrication of aligner. Digital model (A), Virtual tooth movement set-up (B), Physical models produced by FDM 3D printer (C).
Bolton’s analysis indicated a 2-mm excess of the upper anterior teeth because the anterior ratio was 74.5%. Thus, we began the treatment of the upper arch with early slicing. Moreover, a rectangular attachment was added to the labial surface of the upper left lateral incisor for root torque control. After three months of treatment, we observed obvious off-tracking, thus took new dental impressions for the first refinement. After seven and a half months of treatment, the second refinement was performed. The treatment goal was achieved after 11 months of treatment (Figure 4). We used nine aligners for the upper arch and seven for the lower arch. Clear aligner treatment is effective for aligning and levelling teeth, but less effective for certain types of tooth movement, such as rotation and anterior extrusion. In this case, a clear button was bonded to the labial surface of the upper left canine, and an elastic traction was applied from the clear button to the aligner for the canine extrusion (Figure 5).
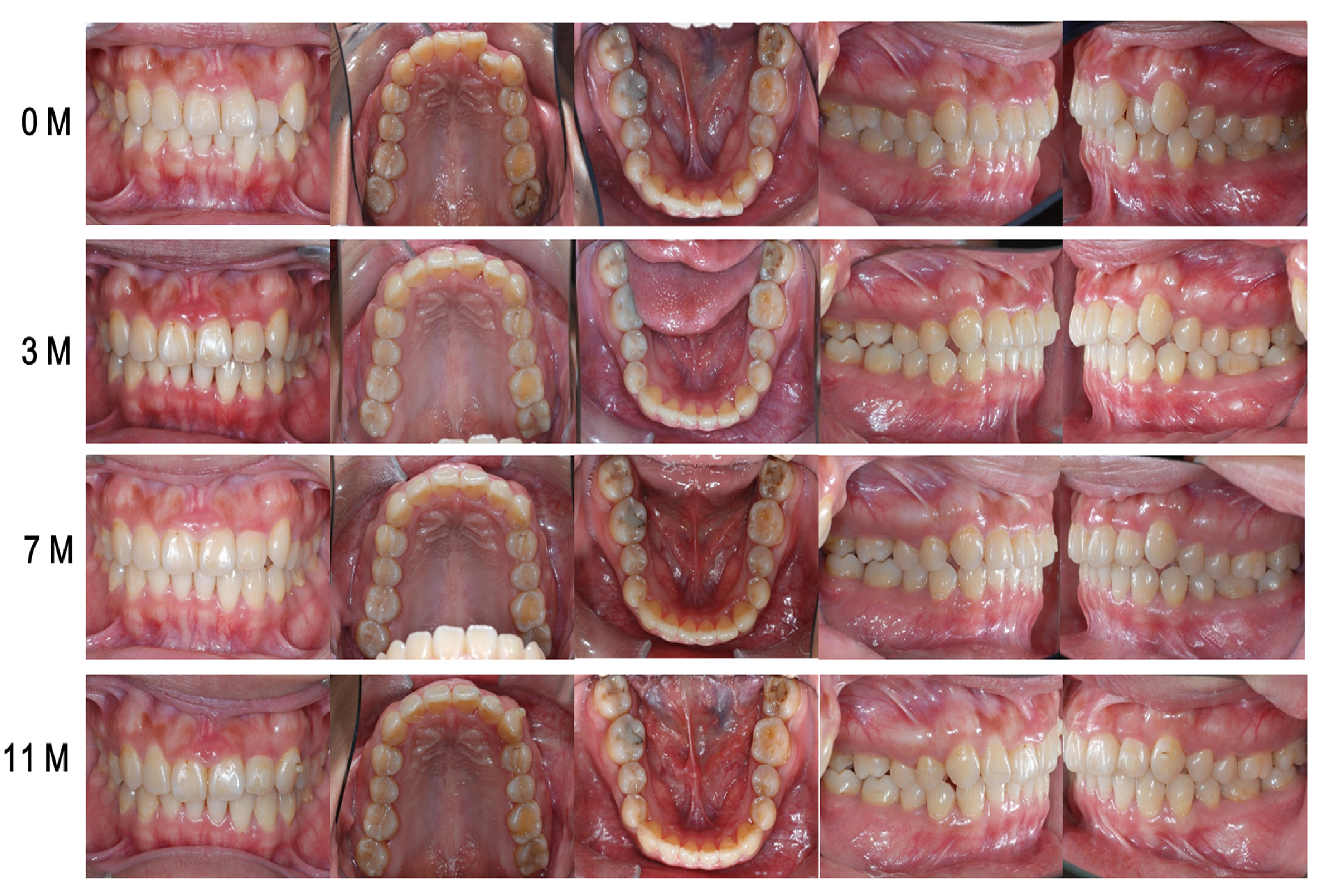
Figure 4: Pre-treatment, progress, and post-treatment intra-oral photographs.
Treatment Results
The anterior tooth alignment significantly improved, and the upper and lower dental midlines were almost coincident (Figure 4). As the cephalometric analysis shows, the upper and lower incisors retracted three to four degrees. The cephalometric superimposition shows an increase in the mandibular plane angle by 1 degree and retraction of the upper and lower lips (data not shown). The upper incisors were retracted 1.5 mm, while the upper right molar was maintained. No pathological change was observed in post-treatment panoramic radiographs (Figure 2). The superimposition of the pre-treatment and post-treatment digital models shows the movement of each tooth in detail, based on the registration area determined by the palatal rugae points for the upper arch and posterior teeth for the lower arch (Figure 5). The buccolingual section views reveals that the upper left lateral incisor moved labially 2.1 mm and the lower left central incisor moved 1.29 mm.
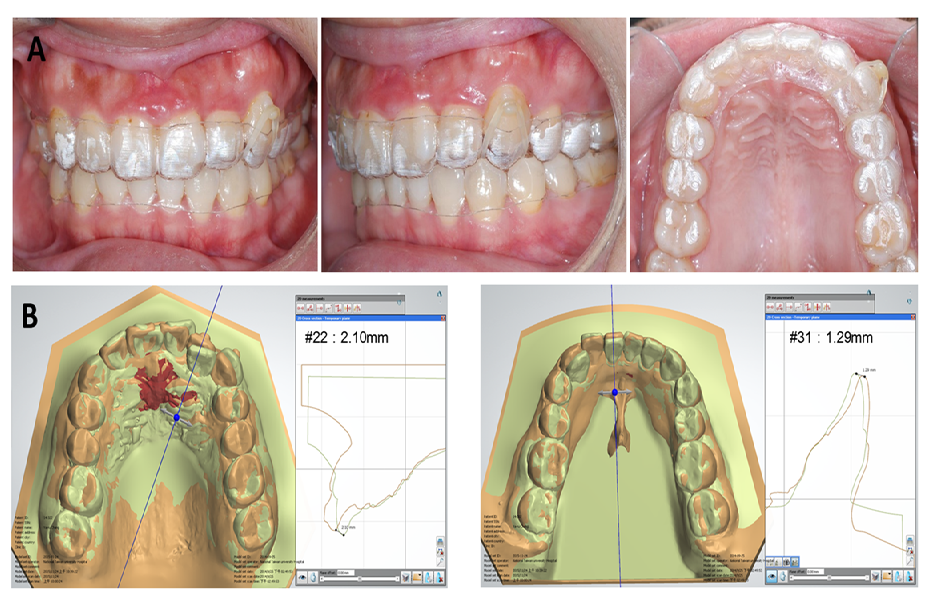
Figure 5: Auxiliaries to clear aligner therapy. Extrusion of upper left lateral canine by elastic traction from clear button to aligner(A), Superimposition of pre-treatment (green) and post-treatment (brown) digital models(B).
Discussion
This case report demonstrates digital orthodontic treatment with clear aligners to correct anterior teeth mal-alignment. Clear aligner treatment has many benefits, including the possibility of engaging the locked-in tooth in the entire force system during the initial stage of treatment. The splint effect from occlusal coverage may lead to intrusion of posterior teeth, facilitating closure of anterior open bite. However, intrusion of posterior teeth increases the treatment difficulty in correcting deep overbite. If posterior open bite occurs, cutting off the posterior part of the aligners to reduce the intrusive force on the molars may be considered. Otherwise, fixed appliances combined with vertical elastics can be used for molar extrusion. In this case, in order to reduce the splint effect of the aligner, we began the treatment for the upper arch only, postponing the treatment of the lower arch until the upper dentition was properly aligned. Moreover, incorporating bite ramps with the aligners produced the bite opening effect, thereby reducing the aligner-induced intrusion of the posterior teeth. In addition, buccally uprighting the lower posterior teeth and improving the curve of Wilson can facilitate bite opening.
Three-dimensional tooth movement set-up of virtual dental models provides a new tool for orthodontics. However, the predicted tooth movement may not occur as expected. Kravitz et al reported that the mean accuracy of tooth movement with Invisalign was 41%, and that 70 - 80% of patients receiving Invisalign required mid-course correction/refinement, or adjunctive fixed appliances to complete the treatment[7]. In a recent study reported by Simon et al., the overall mean efficiency of incisor torque, premolar derotation, and molar distalization using Invisalign was 59%. They investigated 30 consecutive patients and found a mean accuracy of 42% for upper incisor torque, 40% for premolar derotation, and 87% for distalization of upper molars[4]. Chisari et al. conducted a prospective clinical trial to move one central incisor 1 mm over eight weeks, and reported a mean efficiency of 57%[8]. Thus the tooth movement shown by tooth movement simulation software does not accurately predict the actual outcome of the treatment. In digital orthodontic treatment with clear aligners, complete correction of malocclusion often requires mid-course correction.
Composite attachments can be designed to increase retention of aligners and to enhance specific tooth movement. The use of attachments allows for better control of tooth movement and ensures complete tracking with the aligners. Gomez et al. used a 3D finite element model to describe the initial force system of plastic aligners during bodily movement of upper canines with and without composite attachment[9]. They reported that the force system resulting from imposing a distal displacement onto an upper canine with a pair of ellipsoid attachments closely resembles that for bodily tooth movement. The absence of attachments in the simulation of the same displacement produced a force system comparable to uncontrolled tooth inclination. Dasy et al. reported an experiment comparing vertical displacement force of two kinds of attachments (ellipsoid and beveled rectangular attachments), and found that the beveled attachments increase retention significantly compared with ellipsoid attachments or no attachment[10].
Many factors influence the characteristics of force transmitted via the aligners, such as the properties of the materials used, the thickness of the material, the amount of activation, and the use of attachments. Thermoplastic appliances made from thicker materials produce greater force, while appliances that receive greater activation may deliver less force. Simon et al. used a biomechanical measurement system to study the force and moments generated by aligners of the Invisalign system for incisor torque, premolar derotation, and molar distalization[11]. The results suggested that the forces and moments are within the range of orthodontic forces, and premolar derotation has to be supported with an attachment.
Physical replicas of virtual dental models can be constructed using different methods, including subtractive or additive manufacturing[12]. Hazeveld et al. reported that the dental models produced by digital light processing, jetted photopolymer, and three-dimensional printing techniques were clinically acceptable in terms of accuracy and reproducibility, suggesting feasibility for select applications in orthodontics[13]. Fused Deposition Modeling (FDM) is less expensive and easier, and has advantages over other 3D printing methods such as Stereolithography (SLA), which uses a laser to cure liquid photopolymer resins. The FDM 3D printer employs an additive method of laying down thermoplastic material along a programmed X-Y-Z coordinate system. Lee et al. evaluated the accuracy of replica teeth made by FDM and PolyJet technology, and suggested that both technologies are accurate enough to print dental models for use in orthodontic diagnosis and treatment[14]. There are several FDM thermoplastics available, such as Polylactic Acid (PLA) and the petroleum-based plastics, e.g. Acrylonitrile Butadiene Styrene (ABS). PLA has become a very popular choice in 3D printing communities, considering its low toxicity and greater environmental friendliness.
In-office 3D printing makes it possible for orthodontists to print physical models that can be used for fabricating aligners. Fabrication of physical models by FDM 3D printer can reduce cost and improve efficiency of service delivery compared to outsourcing. An in-office 3D printer produces a physical dental model within hours rather than days. Additional time can be saved by printing at night or on weekends. Moreover, orthodontists can modify the settings for tooth movement on virtual models as much as they want, because the cost of making a physical model is not expensive.
Conclusion
Esthetics is the major concern of many orthodontic patients. Clear aligner treatment is more esthetic and comfortable, compared to fixed appliance therapy using conventional brackets. Tooth movement simulation software and in-office 3D printer provides orthodontists with improved options for aligner therapy.
Acknowledge:
This work was partially supported by grant from Ministry of Science and Technology, R.O.C. (MOST 103-2218-E-194-003).
References
- 1. Sheridan, J.J., LeDoux, W., McMinn, R. Essix retainers: fabrication and supervision for permanent retention. (1993) J Clin Orthod 27(1): 37-45.
Pubmed || Crossref || Others - 2. Graber, T.M., Vanarsdal, R.L. Orthodontics: Current principles and techniques, 5 ed. (2012).
Pubmed || Crossref || Others - 3. Rossini, G., Parrini, S., Castroflorio, T., et al. Efficacy of clear aligners in controlling orthodontic tooth movement: a systematic review. (2015) Angle Orthod 85(5): 881-889.
Pubmed || Crossref || Others - 4. Simon, M., Keilig, L., Schwarze, J., et al. Treatment outcome and efficacy of an aligner technique--regarding incisor torque, premolar derotation and molar distalization. (2014) BMC Oral Health 14: 68.
Pubmed || Crossref || Others - 5. Baldwin, D.K., King, G., Ramsay, D.S., et al. Activation time and material stiffness of sequential removable orthodontic appliances. Part 3: premolar extraction patients. (2008) Am J Orthod Dentofacial Orthop 133(6): 837-845.
Pubmed || Crossref || Others - 6. Buschang, P.H., Ross, M., Shaw, S.G., et al. Predicted and actual end-of-treatment occlusion produced with aligner therapy. (2015) Angle Orthod 85(5): 723-727.
Pubmed || Crossref || Others - 7. Kravitz, N.D., Kusnoto, B., BeGole, E., et al. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. (2009) Am J Orthod Dentofacial Orthop 135(1): 27-35.
Pubmed || Crossref || Others - 8. Chisari, J.R., McGorray, S.P., Nair, M., et al. Variables affecting orthodontic tooth movement with clear aligners. (2014) Am J Orthod Dentofacial Orthop 145: 82-91.
Pubmed || Crossref || Others - 9. Gomez, J.P., Pena, F.M., Martinez, V., et al. Initial force systems during bodily tooth movement with plastic aligners and composite attachments: A three-dimensional finite element analysis. (2015) Angle Orthod 85(3): 454-460.
Pubmed || Crossref || Others - 10. Dasy, H., Dasy, A., Asatrian, G., et al. Effects of variable attachment shapes and aligner material on aligner retention. (2015) Angle Orthod 85(6): 934-940.
Pubmed || Crossref || Others - 11. Simon, M., Keilig, L., Schwarze, J., et al. Forces and moments generated by removable thermoplastic aligners: incisor torque, premolar derotation, and molar distalization. (2014) Am J Orthod Dentofacial Orthop 145(6): 728-736.
Pubmed || Crossref || Others - 12. van Noort, R. The future of dental devices is digital. (2012) Dent Mater 28(1): 3-12.
Pubmed || Crossref || Others - 13. Hazeveld, A., Huddleston Slater, J.J., Ren, Y. Accuracy and reproducibility of dental replica models reconstructed by different rapid prototyping techniques. (2014) Am J Orthod Dentofacial Orthop 145(1): 108-115.
Pubmed || Crossref || Others - 14. Lee, K.Y., Cho, J.W., Chang, N.Y., et al. Accuracy of three-dimensional printing for manufacturing replica teeth. (2015) Korean J Orthod 45(5): 217-225.
Pubmed || Crossref || Others










