
Congenital Ovarian Cyst: Diagnosis and Perinatal Management
Ricardo Pérez¹, Ana Pomares², Coral Bravo², Francisco Gámez¹, Ãngel Aguarón¹, Luis Ortiz¹,
Affiliation
1Department of Obstetrics and Gynecology, Hospital General Gregorio Maranon, Universidad Complutense de Madrid, Spain
2Department of Obstetrics and Gynecology, Hospital Central de la Defensa Gomez Ulla, Universidad de Alcala de Henares. Madrid, Spain
Corresponding Author
De León-Luis, J. Department of Obstetrics and Gynecology, Fetal Medicine Unit, Hospital General Gregorio Maranon, Universidad Complutense de Madrid, Spain. Tel: 34(91)5290218; E-mail: jdeleonluis@yahoo.es
Citation
Pérez, R., et al. Congenital ovariancyst: diagnosis and perinatal management (2015) J Gynecol Neonatal Biol 1(1): 1-5.
Copy rights
©2015 Leon-Luis, J.D. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Fetal intraabdominal cyst; Fetal intraabdominal mass; Fetal ovarian cyst; Fetal ovarian torsion
Abstract
Objective: To describe prenatal and postnatal outcomes of ultrasonographically diagnosed fetal ovarian cysts (FOC) and to review the literature to propose an obstetric management algorithm.
Methods: We performed a retrospective analysis of fetuses with an ultrasound-based diagnosis of FOC. The size, location, and ultrasound features of the cysts were recorded. Follow-up and treatment modalities are described.
Results: 13 of 16 had follow-up data. Almost all cases were diagnosed in the third trimester. FOC was mostly unilateral, with a mean diameter of 40.4 mm. The cysts were classified as simple in 12 cases (75%). Eleven cases (68.7%) remained stable, and 2 resolved spontaneously (12.5%) during pregnancy. No associated anomalies or chromosomal abnormalities were found. Postnatal management was surgical in 50% of cases, with laparoscopy as the main procedure. Cystectomy and alpingo-oophorectomy were performed in 4 infants each.
Conclusions: FOC is frequently isolated. Prognosis is generally good. Regular ultra-sound is necessary before and after birth to detect complications that could endanger the ovarian parenchyma. Conservative management is recommended in simple cysts under 4cm, and surgical procedures can be performed in larger simple cysts or when complications are suspected. Tissue-sparing surgery is preferable.
Introduction
Fetal ovarian cysts (FOC) are the second most common type of abdominal mass after urinary tract mass and the most common abdominal mass in female newborns[1]. In most cases, FOC are small, unilateral, benign, and asymptomatic and regress spontaneously during gestation or during the first months of life[2,3]. However, complications such as intracystic hemorrhage and ovarian torsion can occur and could lead to complete loss of the ovarian parenchyma[4].
The first neonatal ovarian cyst was reported in 1889 as an autopsy finding in a stillborn infant[5], but the first sonographic diagnosis of FOC was made in 1975[6]. Since then, improvements in ultrasound techniques and protocol-based systematic examination of fetal anatomy have led to an increase in the number of cases of FOC detected. Nevertheless, management remains controversial for several reasons[7]. First, the differential diagnosis between FOC and other fetal abdominal cystic masses can be challenging[3]. Second, in the case of complicated cysts, findings supporting conservative and invasive management are contradictory[8]. Finally, treatment of the neonate also differs between the reported series[9,10].
The aims of the present study were to evaluate our findings in the management and follow-up of prenatally diagnosed FOC and to design a treatment algorithm that could help clinicians to better address this anomaly.
Materials and Methods
We performed a descriptive observational study of all patients with a prenatal ultrasound-based diagnosis of FOC in our Fetal Medicine Unit from October 2004 to September 2011. All ultrasound examinations were performed transabdominally using a 4-8–MHz probe (GE Logic 9 and Voluson Expert).
Gestational age was confirmed based on the date of the last menstrual period or by measurement of the fetal crownrump length in the first trimester ultrasound evaluation. Irrespective of gestational age, a diagnosis of FOC was confirmed when a cystic mass was identified in a female fetus, mainly in the lower part of the abdomen. This mass had to be distinct from the bladder and more than 20 mm in diameter (Figure 1). According to the Nussbaum classification[11]. FOC were classed as simple or uncomplicated and complex or complicated by torsion or hemorrhage. An uncomplicated cyst is anechoic, with a thin wall. A complicated cyst contains fluid-debris level, retracting clot, septa and often has a thick wall[11]. Exhaustive fetal ultrasound was performed after the diagnosis of FOC in order to detect any associated anomalies. Follow-up was with serial ultrasound every two weeks to detect signs of a growing cyst or complications such as intracystic hemorrhage or torsion of the mass.
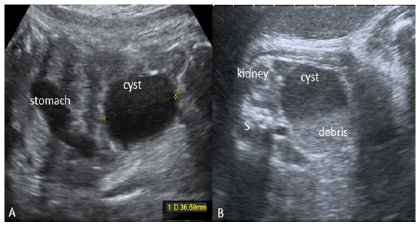
Figure 1: Ultrasound images of fetal ovarian cysts.
A. Longitudinal view of fetal abdomen showing a simple ovarian cyst.
B. Axial view of the fetal abdomen showing a complex ovarian cyst with internal debris. S, spine.”
The potential need for neonatal surgery was taken into consideration, even though no prenatal procedures were performed in our unit thus we did not consider in utero aspiration in any case. Karyotype studies were only suggested if FOC was associated with markers of aneuploidy and/or other congenital disorders related to chromosomal abnormalities. Maternal-fetal variables and perinatal data were obtained retrospectively from the medical records. Transabdominal ultrasound was performed on all newborns with prenatal diagnosis of FOC.
Results
We found 16 cases of FOC during the study period in a total of 57,934 newborns in our center of which 48.4% were female (incidence 5.7/10,000 female newborns). (Table 1) summarizes prenatal and postnatal clinical variables and sonographic and histological findings. The mean gestational age at diagnosis was 32 weeks (±5 weeks). All cases were diagnosed in the third trimester, except for 1 case, which was detected at 16 weeks during an amniocentesis for high risk in the combined screening. FOC were mostly unilateral and diagnosed with a mean diameter of 40.4 mm (±17.1 mm). In 11 cases (68.7%), the size of the FOC remained stable during pregnancy. However, 5 cysts became enlarged, with the result that the mean maximum diameter at the end of gestation was 45.7 mm (±17.7 mm). Only 2 simple cysts resolved spontaneously during pregnancy (12.5%), and no simple cysts became complex prenatally. Most cysts (12/16, 75%) were classed as simple according to the Nussbaum classification[11]. All the cysts were isolated, with no associated anomalies or markers of chromosomal abnormalities. All the pregnancies were unremarkable and most were full-term. Delivery was vaginal, and fetal weight was in the normal range. Relevant findings are shown in (Table 1).
Postnatal follow-up was managed by pediatricians and pediatric surgeons, and data were collected for 13 cases (3 cases were lost to follow-up). Perinatal management was conservative in 5 cases (38.4%) the cyst resolved spontaneously after birth and surgical in 8 cases (61.5%). Surgery was indicated for complex cysts (2 cases), or specific symptoms and signs (e.g. pain, abdominal distension) suggesting ovarian torsion (6 cases). Most of the procedures were performed by laparoscopy within the first 15 days after birth. Laparoscopic cystectomy and salpingo-oophorectomy were performed in 4 cases each. Histopathology revealed benign ovarian cyst in all the 8 cases.
Table 1: Ultrasound features and clinical management in 16 cases of fetal ovarian cyst.
| 1 | 34 | Right | 64 | Simple | 37 | Vaginal | 2900 | Surgical (2 days) | Laparoscopic cystectomy | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 | 30 | Left | 26 | Simple | 33 | CS | 2760 | IUGR of the nonaffected twin | -- | -- | -- |
| 3 | 30 | Right | 27 | Complex | 39 | Vaginal | 2850 | Conservative | -- | -- | |
| 4 | 34 | -- | 81 | Complex | 39 | Vaginal | 3040 | Surgical (7 days) | Laparoscopic cystectomy | Not available | |
| 5 | 38 | - | 46 | Complex | 38 | Vaginal | 3200 | Surgical (2 days) | Laparoscopic cystectomy | BOC Necrosis | |
| 6 | 35 | left | 38 | Simple | 39 | Vaginal | 3690 | Bilateral | Surgical (6 months) | Laparotomy L: detorsion + cystectomy R: salpingo-oophorectomy |
Bilateral haemorrhagic cysts |
| 7 | 43 | left | 50 | Complex | 39 | Vaginal | 3360 | Surgical (15 days) | Laparoscopic salpingooophorectomy | BOC Necrosis | |
| 8 | 35 | Right | 45 | Simple | 39 | Vaginal | 3080 | Conservative | - | - | |
| 9 | 35 | left | 33 | Simple | 36 | CS | 2880 | Surgical (3 months) | Laparoscopic oophorectomy | BOC Necrosis | |
| 10 | 34 | Right | 48 | Simple | 40 | Vaginal | 2960 | - | - | - | |
| 11 | 16 | Right | 38 | Simple | 39 | Vaginal | 3890 | Gestational diabetes | Conservative | - | - |
| 12 | 33 | Right | 80 | Simple | 40 | Vaginal | 3170 | Patent FO Congenital torticollis | Surgical (2 days) | Laparoscopic salpingooophorectomy and appendicectomy | BOC Necrosis Congestive appendix |
| 13 | 31 | Right | 23 | Simple | 37 | Vaginal | 3250 | Conservative | - | - | |
| 14 | 30 | Left | 28 | Simple | 40 | Vaginal | 3660 | - | - | - | |
| 15 | 36 | left | 50 | Simple | 40 | Vaginal | 3000 | Genital autostimulation | Conservative | - | - |
| 16 | 36 | Right | 55 | Simple | 39 | Vaginal | 3220 | Surgical (8 days) | Laparoscopic salpingooophorectomy | Hemorrhagic cyst |
BOC, benign ovarian cyst; CS, cesarean section; FO, foramen oval; IUGR, intrauterine growth restriction; L, left; R, right; US, ultrasound.
Discussion
FOC is reported to be the most common abdominal mass in the female fetus (incidence 1 in 2500 live births)[12]. Our findings confirm this incidence (1/1755 female newborns).
Ultrasound diagnostic criteria include the following: (1) confirmation of female gender;(2) presence of a cystic structure that is regular in shape and located off the midline; (3) size ≥ 20 mm in diameter (otherwise the diagnosis is maturing follicles); (4) identification of normal urinary tract anatomy; and (5) identification of normal gastrointestinal structures[13].
FOC is mostly diagnosed in the third trimester (≥28 weeks), and the cyst is usually small (< 40 mm) and unilateral (95%). These findings are consistent with our results[14]. The origin of FOC is unclear, although the cyst may develop as a result of fetal ovarian stimulation by hormones such as fetal follicle-stimulating hormone, maternal estrogens, and placental human chorionic gonadotropin[15]. Incidence is higher in pregnancies complicated by Rhesus factor incompatibility, preeclampsia, and diabetes mellitus, presumably because of the increased production of human chorionic gonadotropin by a large placenta[16]. Fetal hypothyroidism and congenital adrenal hyperplasia are other possible causes[17].
Cyst echogenicity is the main criteria for establishing prognosis of FOC. Nussbaum et al. categorized FOC according to ultrasound criteria as simple (uncomplicated or follicular) and complicated[11]. Simple cysts are anechogenic, round, unilocular, intrapelvic, or more often intra-abdominal, unilateral or seldom bilateral, thin-walled, and more or less mobile with the mother’s position. Complicated cysts, on the other hand, are het-erogeneous and thick-walled, with hyperechogenic components. They contain free floating material with intracystic septa and are mobile after torsion. In fact, the absence of color Doppler flow is highly specific for ovarian torsion[18].
In order to facilitate differential diagnosis, Lee et al.[19] described a sonographic sign called the “daughter cyst”, which consists of a small (2-8 mm), round, anechogenic structure resembling a small cyst within or outside the main cyst. This feature confirmed the ovarian origin of the cysts, with a sensitivity of 82% and specificity of 100%[19]. We did not assess this sign. (Table 2) describes the differential diagnosis and management of fetal abdominal cystic masses.
Table 2: Differential diagnosis of fetal intra-abdominal cystic masses.
| Origin | Location | Ultrasound features | Associations | Evolution |
|---|---|---|---|---|
| Intestinal | ||||
| Mesenteric cyst | Intestinal | Thick wall Heterogeneous | Obstruction | Surgery if symptomatic or complicated |
| Duplication | Ileum | Tubular structure parallel to intestine | Split notochord Other associated anomalies | Surgery if symptomatic or complicated |
| Meconium pseudocyst | Intestinal | Hyperechogenic ring | Obstruction | Spontaneus resolution |
| Duodenal atresia | Intestinal midline | “Double bubble” sign | Associated with Down syndrome, Meckel diverticulum | Surgery |
| Urinary tract | ||||
| Renal cyst | Peripheral | Enlarged kidney | Pottersyndrome, renal insufficiency, oligohydramnios | Good prognosis if pulmonary hypoplasia is ruled out |
| Urachal cyst | Anterior midline | Connected to bladder | - | Good prognosis |
| Urinary obstruction cyst | Bilateral | Hyperechogenic renal parenchyma Dilated urinary tract | Urinary tract obstruction | Surgery |
| Genital | ||||
| Hydrocolpos | Midline | Sebaceous cystcontents, unilocular, acoustic shadowing | Surgery | |
| Cystic ovarian torsion with AA and migration | Pelvis | Complex cyst | Loss of ovarian function | Surgery |
| Other | ||||
| Anterior eningocele | Midline | Mass Bony deffect | Other neurologic anomalies | Surgery |
| Lymphangioma | Cervical, axillary mediastinal, mesenteric, abdominal | |||
A review of the literature revealed that most FOC are benign, being carcinomas very uncommon (< 3%)[19]. In our study, histopathology revealed that all the cysts were benign.
Fetal complications are infrequent but several have been described. Hydramnios appears in 10% of pregnancies with FOC, especially when cysts are larger than 50-60mm. Hydramnios and ascites can be secondary to partial gastrointestinal tract obstruction[12,20]. However, we did not observe these conditions in our series.
Ovarian torsion is the most common and serious adverse condition of FOC and may manifest as fetal tachycardia owing to peritoneal irritation[21,22]. Ultrasound findings of adnexal torsion are not specific, but bleeding within an ovarian cyst is usually associated with torsion[23]. Torsion can be further complicated by circulatory impairment and hemorrhagic infarction with or without autoamputation[24]. The amputated ovary is then resorbed or becomes a mobile calcified abdominal mass[24].
Other rare complications include gastrointestinal obstruction or perforation, urinary tract obstruction, incarcerated inguinal hernia, ovarian autoamputation, and sudden infant death[2].
FOC is frequently solitary and not associated with chromosomal defects[25]. Nevertheless, several anomalies, such as hypertrophic pyloric stenosis, corpus callosum agenesis, and fetal hypothyroidism have been reported to be associated with FOC[20] In our series, all the FOC were isolated.
Prenatal detection and prenatal and postnatal follow-up of FOC is mainly based on ultrasound, however fetal or neonatal magnetic resonance imaging may be useful and should be performed when ultrasound does not provide definitive information or when serial ultrasound examinations do not show spontaneous regression of an ovarian cyst[26].
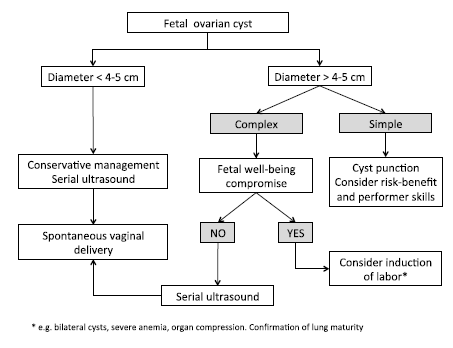
Management is controversial with several options described in the literature, including watchful expectancy, antenatal aspiration of simple cysts to prevent torsion and ovarian loss and finally, observation or resection of all complex cysts in the neonatal period[27]. Prenatally, FOC often regress spontaneously requiring exclusively periodical follow-up. Other cases persist after birth and may eventually develop complications thus FOC need to be monitored prenatally and postnatally by serial ultrasound[25,28]. A period of two weeks was considered reasonable in our center for prenatal follow-up.
In the rare event of bilateral FOC or fetal severe anaemia due to rupture of the cyst or fetal compromise secondary to compression, early delivery should be considered, after confirmation of fetal lung maturity, to prevent fetal distress or the possibility of bilateral ovarian loss[2].
In utero aspiration of simple FOC may be considered in simple ovarian cysts larger than 4-5 cm in order to reduce their size and avoid complications such as torsion or compression[8]. Several authors have shown the technique can be safe and effective in preventing ovarian torsion, as well as giving hope of fertility to the newborn[8]. However, Heling et al. only recommend it if the cyst is large enough to impair spontaneous delivery or cause distension of the fetal abdomen[4], as this procedure is associated with complications such as reformation of the cyst, infection, premature rupture of membranes and premature labor. In our center, we did not perform aspiration in any of our cases.
Based on the management options previously described we have developed an algorithm for the prenatal approach of FOC (Figure 2).
Postnatally, many authors have advocated conservative management of asymptomatic simple and complex FOC based on the limited risks of this approach compared to the complications of a surgical procedure and a general anesthesia[29], On the contrary, Karakus et al. reported that complex ovarian cysts lead to problems even after regression in the postnatal period and require operative intervention sooner or later. The literature reveals postnatal surgery by sparing procedure has been recommended for cysts that are complex, irrespective of their size[21] in order to avoid the loss of the ovary and infertility[3]. When neonatal ovarian cysts cause pain, vomiting, fever, irritability, and abdominal distention then surgical procedure is clearly justified.
Minimally invasive approaches, such as laparoscopic and microendoscopic procedures are recommended[3], since they allow aspiration, cystectomy, decapsulation of the ovary, stripping of the cyst wall, and, if necessary, oophorectomy. Mini-laparotomy with externalization-aspiration has been shown to be safe, with similar advantages to laparoscopy[30].
In our series, surgery was indicated in 8 cases (50%). Laparotomy was performed in the only case of bilateral cysts and detorsion and cystectomy of the left ovarian and salpingo-oophorectomy of the right ovarian were needed. Oophorectomy was performed because of intracystic hemorrhage or necrosis of the ovary in other 4 cases.
The benefits of surgical management include removal of the cyst for optimal preservation of the ovary, histological confirmation, and division of any adhesions between the ovary and adjoining organs[9].
Vaginal delivery is recommended if no obstetric contraindications are present[30].
Conclusion
FOC is a rare anomaly that usually presents in isolation. However, differential diagnosis including other fetal cystic masses is essential. Appropriate management depends on the size of the cyst and the presence of complications. Conservative prenatal and postnatal management is the main recommendation for uncomplicated cysts. When surgery is necessary, minimally invasive procedures are the most suitable for preservation of the ovarian parenchyma and treatment of complications such as ovarian torsion.
Acknowledgement: The authors are grateful to Mr. Thomas O’Boyle for editorial assistance.
Disclosure: There is absence of any interest to disclose.
References
- 1. Meizner, I., Levy, A., Katz, M., et al. Fetal ovarian cysts: pre-natal ultrasonographic detection and postnatal evaluation and treatment. (1991) Am J Obstet Gynecol 164(3): 874- 878.
- 2. Bornstein, E., Barnhard, Y., Ferber, A., et al. Acute progression of a unilateral fetal ovarian cyst to complex bilateral cysts causing acute polyhydramnios. (2006) J Ultrasound Med 25(4): 523- 526.
- 3. Akin, M.A., Akin, L., Ozbek, S., et al. Fetal-neonatal ovarian cysts-Their monitoring and management: retrospective evaluation of 20 cases and review of the literature. (2010) J Clin Res Pediatr Endocrinol 2(1): 28- 33.
- 4. Heling, K.S., Chaoui, R., Kirchmair, F., et al. Fetal ovarian cysts: prenatal diagnosis, management and postnatal outcome. (2002) Ultrasound Obstet Gynecol 20(1): 47- 50.
- 5. Doran, A.H. Large ovarian tumors in 7 months old child. London: Trans. Path. (1889) Soc.
- 6. Valenti, C., Kassner, G., Yermakow, V., et al. Antenatal diagnosis of a fetal ovarian cyst. (1975) Am J Obstet Gynecol 123: 216.
- 7. Comparetto, C., Giudici, S., Coccia, M.E., et al. Fetal and neonatal ovarian cysts: what's their real meaning? (2005) Clin Exp Obstet Gynecol 32(2): 123- 125.
- 8. Noia, G., Visconti, D., Pellegrino, M., et al. Invasive fetal therapies: approach and results in treating fetal ovarian cysts. (2012) J Matern Fetal Neonatal Med 25(3): 299- 303
- 9. Monnery-Noche, M.E., Auber, F., Jouannic, J.M., et al. Fetal and neonatal ovarian cysts: is surgery indicated? (2008) Prenat Diagn 28(1): 15- 20.
- 10. Galinier, P., Carfagna, L., Juricic, M., et al. Fetal ovarian cysts management and ovarian prognosis: a report of 82 cases. (2008) J Pediatr Surg 43(11): 2004- 2009.
- 11. Nussbaum, A.R., Sanders, R.C., Hartman, D.S., et al. Neonatal ovarian cysts: sonographic-pathologic correlation. (1988) Radiology 168(3): 817- 821.
- 12. Bryant, A.E., Laufer, M.R. Fetal ovarian cysts: incidence, diagnosis and management. (2004) J Reprod Med 49(5): 329- 337.
- 13. Kwak, D.W., Sohn, Y.S., Kim, S.K., et al. Clinical experiences of fetal ovarian cyst: diagnosis and consequence. (2006) J Korean Med Sci 2006 21(4): 690- 694.
- 14. Sheth, R., Hoelzer, D., Scattergood, E., et al. In utero fetal ovarian torsion with imaging findings on ultrasound and MRI. (2012) Case Rep Radiol 2012: 151020.
- 15. Nguyen, K.T., Reid, R.L., Sauerbrei, E. Antenatal sonographic detection of a fetal theca lutein cyst: a clue to maternal diabetes mellitus. (1986) J Ultrasound Med 5(11): 665- 667.
- 16. Vogtlander, M.F., Rijntjes-Jacobs, E.G., van den Hoonaard, T.L., et al. Neonatal ovarian cysts. (2003) Acta Paediatr 92: 498.
- 17. Mudholkar, V.G., Acharya, A.S., Kulkarni, A.M., et al. Antenatally diagnosed neonatal ovarian cyst with torsion. (2011) Indian J Pathol Microbiol 54(1): 228- 229.
- 18. Coulson, C.C., Kasales, C.J., Devi, G. Antenatal doppler diagnosis of fetal ovarian torsion. (2000) Obstet Gynecol 95(6 Pt 2): 1039.
- 19. Lee, H.J., Woo, S.K., Kim, J.S., et al. "Daughter cyst" sign: a sonographic finding of ovarian cyst in neonates, infants, and young children. (2000) AJR Am J Roentgenol 174(4): 1013- 1015.
- 20. Heaton, T.E., Liechty, K.W. Postnatal management of prenatally diagnosed abdominal masses and anomalies. ( 2008) Prenat Diagn 28(7): 656- 666.
- 21. Erol, O., Büyükkınacı, E.M., Sıtkı İsenlik, B., et al. Prenatal diagnosis of fetal ovarian cyst: case report and review of the literature. (2013) J Turkish-Ger Gynecol Assoc 14(2): 119- 122.
- 22. Singal, A.K., Vignesh, K.G., Paul, S., et al. Antenatally diagnosed ovarian cyst with torsion managed laparoscopically. (2008) Journal of Indian Assoc Pediatr Surg 13(1): 28- 29.
- 23. Rha, S.E., Byun, J.Y., Jung, S.E., et al. CT and MR imaging features of adnexal torsion. (2002) Radiographics 22(2): 283- 294.
- 24. Currarino, G., Rutledge, J.C. Ovarian torsion and amputation resulting in partially calcified, pedunculated cystic mass. (1989) Pediatr Radiol 19(6-7): 395- 399.
- 25. Sanchez, P., Gamez, F., de Leon-Luis, J., et al. Fetal ovarian cyst: prenatal diagnosis, perinatal outcome and treatment. Case series and literature review. (2012) Ginecol Obstet Mex 80(2): 84- 90.
- 26. Nemec, U., Nemec, S.F., Bettelheim, D., et al. Ovarian cysts on prenatal MRI. (2012) Eur J Radiol 81(8): 1937- 1944.
- 27. Amodio J, Hanano A, Rudman E, Banfro F, Garrow E. Complex left fetal ovarian cyst with subsequent autoamputation and migration into the right lower quadrant in a neonate: case report and review of the literature. (2010) J Ultrasound Med 29(3): 497- 500.
- 28. Turgal, M., Ozyuncu, O., Yazicioglu, A. Outcome of sonographically suspected fetal ovarian cysts. (2013) J Matern Fetal Neonatal Med 26(17): 1728- 1732.
- 29. Nakamura, M., Ishii, K., Murata, M., et al. Postnatal Outcome in Cases of Prenatally Diagnosed Fetal Ovarian Cysts under Conservative Prenatal Management. (2015) Fetal Diagn Ther. 37(2): 129- 134.
- 30. Ferro, F., Iacobelli, B.D., Zaccara, A., et al. Exteriorization-aspiration minilaparotomy for treatment of neonatal ovarian cysts. (2002) J Pediatr Adolesc Gynecol 15(4): 205- 207.










