
Correlation Between Tempromandibular Disorder and Fixed Partial Denture & Restorative Treatment
Mohammad Alomair1, Waleed Alshaman1*, Mohammad Alshammary2, Magdy K Hamam3, Hamad N. Albagiah3
Affiliation
- 1Ministry of health, Dental sector, Tabuk, Saudi Arabia
- 2Ministry of health, Dental sector, Hail, Saudi Arabia
- 3College of Dentistry, King Saud University, Saudi Arabia
Corresponding Author
Waleed Alshaman, Ministry of health, Dental sector, Tabuk, Saudi Arabia, E-mail: alshaman@hotmail.com
Citation
Alshaman, W., et al. Correlation between Temporomandibular Disorder, Fixed Partial Denture and Restorative Treatment. (2016) J Dent Oral Care 2(3): 1- 9.
Copy rights
© 2016 Alshaman, W. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Temporomandibular disorders (TMD), Fixed partial denture(FPD), Restorative treatment (RT)
Abstract
The Temporo Mandibular Disorders (TMD) is complex multifactorial problem. It is common cause of orofacial pain problems. The main approach for treatment is supportive therapy. Therefore, the aim of this investigation is to study the effect of fixed partial denture (FPD) and restorative treatment on TMD. A cross sectional survey was conducted in governmental and private hospitals in Riyadh city. A total of 300 patients were enrolled in this survey. The results revealed significant correlation between FPD and restorative treatment, and TMD.
Introduction
According to the Guidelines of the American Academy of Orofacial Pain Temporomandibular disorders (TMD) is defined as, ‘a collective term embracing a number of clinical problems that involve the masticatory musculature, the temporomandibular joints and associated structures, or both[1,2]. Temporomandibular disorders have been recognized as a common orofacial pain condition. The American Dental Association in 1983 has suggested that the term Temporo Mandibular Disorders (TMD) refers to a group of disorders characterized by: pain in the Temporo Mandibular Joint (TMJ), the periauricular area, or the muscles of mastication; TMJ noises (sounds) during mandibular function; and deviations or restriction in mandibular range of motion[3]. The etiology of TMD has been considered to be one of the most controversial issues in clinical dentistry. A majority of dental practitioners believe that occlusal disturbances can cause or are closely related to TMD, and many therefore also include occlusal adjustment as an initial treatment for TMD, whereas most TMD experts hold opposing views[4-6]. Restorative procedures are divided into two types-. (1) Operative and (2) fixed prosthodontic. Operative procedures are those in which the final restorations are fabricated intrao-rally (e.g., an amalgam, a composite resin). Fixed prosthodontic procedures are those that involve extraoral fabrication with final adjustment and cementation in the mouth (e.g., inlays, onlays, full crowns, fixed partial dentures[7]. The prevalence of TMD is still not well known and more studies and comparisons are necessary to allow better understanding of the pathological aspects so as to address effective preventive and therapeutic measures. Few studies reported the prevalence of TMD in Saudi Arabia in normal permanent dentition and adults[8,9]. If your teeth don’t meet evenly, such as when you have a new filling or crown that is slightly “high”, this could cause pain on biting or with extremes of temperature. In the long term you could develop mobile teeth, receding gums, fractures, abnormal wear, tension headaches and even jaw joint problems such as stiffness, clicking and locking (British academy of restorative dentistry). A review of the scientific literature reveals that five major factors associated with TMDs. These factors are the occlusal condition, trauma, emotional stress, deep pain input, and parafunctional activities[10]. Three general classes of record are used for transferring maxilla-mandibular relationships from the patient to the articulator including Interocclusal and hinge axis records. As well as, the graphic records[11]. The reproducibility of occlusal marking technique is low. In studying the influence of force and jaw position on the number of tooth contacts, most restorative procedures cannot be performed without influencing to some degree the existing occlusal condition. The potential effect of restorative procedures on the occlusion is obvious when a complete reconstruction of the dentition is being considered. However, one should be aware that even an occlusal amalgam can have a significant effect on the occlusion when the restoration is undercarved or over carved[12-14].
The observation that many subjects have “occlusal abnormality” without TMD has clearly encouraged reviewers to conclude that occlusal factors have no significant etiological role[2,15]. Results of experimental interference studies are also seen as strong evidence for the same conclusion[16]. The hypothesis, “dental occlusion plays a significant causal role in temporomandibular disorders”, has been a central point of contention for many decades in the attempt to understand these disorders. Recently, certain authors have asserted that the scientific literature does not support this hypothesis determining the cause(s) of TMDs is far from a straightforward and simple process. There is general agreement that TMD is a broad, generic term that encompasses a wide variation of conditions involving the masticatory musculoskeletal structures. There is also wide agreement that causation related to TMDs is of multi factorial origin. The likelihood of identifying any single “cause” as having a predominant role is clearly remote. The aim of this research is to show the relationship between the occlusal interference with fixed prosthesis, restorations, and tempromandibular disorder.
Materials and Methods
Study Population
Request for ethical Approval for this study will be made by applying to College of Dentistry Research Center. The target population this study is male patients attending one governmental and one private hospital in Riyadh The age range for these patients will be limited to age (18 – 70 years old). The patient will identify in undergraduate clinics, intern and post graduate clinics. All of the patient must have a FPD & restorations.
Questionnaire
The questionnaire to be used in this study will be in Arabic. The questionnaire it will determine if there is a correlation between TMD, FPD & restorations. Firstly, the following information was collected: the demographic information such as patient’s age, education, employment status, parity, and economic status .then the past dental history data were collected including some medical relevant as (did you have any medical problem, did have any complication with dental treatment, did you take any medications, etc). The last part is the relation between TMD, FPD & restoration. We focused on the questions about the history of TMD and if there are complications occurred after the prostho-opreative treatment. For example did you have any clicking or deviation or pain in your joint? yes/no .as we mention all the patient must have crowns or FPD or restoration, then the next questions it will be (when they do the treatment, how many crowns he have, any differentiations between the treatment, if its high, if they feel pain in muscle and jaw after treatment etc).
Questionnaire Administration
The questionnaires were initially tested for clarity and accuracy on a sample of 100 male patients. After making necessary changes in the tested questionnaire, the questionnaire were given to supervisor of the clinic in DUC and also to the private clinic. A total of 300 male patients investigated in this study.
Data Analysis
All the collected data were statistically analyzed using SPSS version 21 software. The Chi square tests were used to determine the significant relations.
Results
Table 1 shows that the distribution of the study sample according to the variable Age that the vast majority (217) of the study sample, representing a rate of (72.3%) of the total study sample age (from 20 to less than 25 years old), while it was found that (29) of the study sample, representing a rate of (9.7%) of the total study sample age (from 25 to less than 30), also found that (12) of the study sample, representing a rate of (4%) of the total study sample age ( from 35 to less than 40 years old ), while equal proportion of the study sample holders ages (less than 20 years old, from 30 to less than 35 years, from 50 years and above ) and that by (3%) of the total study sample, while it was found that ( 8) of the study sample, representing a rate of (2.7%) of the total study sample age (from 40 to less than 45 years) and finally found that (7) of the study sample, representing a rate of (2.3%) of the total study sample age ( from 45 to less than 50 years).
Table 1: Distribution of the study sample according to the variable Age.
| Age | Sample Size (n) | Percentage |
|---|---|---|
| Less than 20 years | 9 | 3.0% |
| From 20 to less than 25 | 217 | 72.3% |
| From 25 to less than 30 years | 29 | 9.7% |
| From 30 to less than 35 | 9 | 3.0% |
| From 35 to less than 40 | 12 | 4.0% |
| From 40 to less than 45 | 8 | 2.7% |
| From 45 to less than 50 | 7 | 2.3% |
| From 50 and more | 9 | 3.0% |
| Total | 300 | 100% |
Table 2 show that distribution of the study sample according to the variable work, it shows that the vast majority (240) of the study sample, representing a rate of (80%) of the total sample individuals (students), while it was found that (17) of the study sample representing a rate of (5.7%) of the total study sample employed in the police, while it was found that (15) of the study sample, representing a rate of (5%) of the total study sample employed in government jobs, also found that (5) of the study sample representing a rate of (1.7%) of the total study sample teachers , while it was found that (4) of the study sample representing (1.3%) of the total study sample, “doctors”.
Table 2: Distribution of the study sample according to the variable work.
| Job title | Sample Size (n) | Percentage |
|---|---|---|
| Criminal evidence | 1 | 0.3% |
| National guard | 1 | 0.3% |
| Police | 17 | 5.7% |
| Traffic | 1 | 0.3% |
| Provisional institute | 1 | 0.3% |
| Imam University | 1 | 0.3% |
| Businessman | 3 | 1.0% |
| Driver | 2 | 0.7% |
| Student | 240 | 80.0% |
| Doctor | 4 | 1.3% |
| Worker | 1 | 0.3% |
| Military | 1 | 0.3% |
| Private sector | 2 | 0.7% |
| Retired | 1 | 0.3% |
| Financial monitor | 11 | 0.3% |
| Supervisor | 0.3% | |
| Commissioner | 1 | 0.3% |
| Teacher | 5 | 1.7% |
| Engineer | 1 | 0.3% |
| Governmental employee | 15 | 5.0% |
| Total | 300 | 100% |
From Table 3, it is indicated that (0.3%) of the total study sample complain of neurological disorders, while it was found that (0.7%) of the total study sample complain of musculoskeletal disorders, arthritis, also found that (2.3%) of the total study sample complain of psychological pressure, and finally found that (3.3%) of the total study sample complain (stomach pain, headaches, anemia, Orthodontic, disability, asthma, ligamentin the knee).
Table 3: Distribution of the study sample according to medical problems.
| Do you suffer from the following diseases | Yes | No | ||
|---|---|---|---|---|
| Sample Size (n) | Percentage | Sample Size (n) | Percentage | |
| Neurological disorders | 1 | 0.3% | 299 | 99.7% |
| Musculoskeletal disorders – Arthritis | 2 | 0.7% | 298 | 99.3% |
| Psychological pressure | 7 | 2.3% | 293 | 97.7% |
| Medical problem not listed above (stomach pain, headaches, anemia, Orthodontic, disability, asthma, ligament in the knee). | 10 | 3.3% | 290 | 96.7% |
Seen from Table 4 the distribution of the study sample according to the number of combinations or restorations that have shown that (118) of the study sample, representing a rate of (39.3%) of the total members of the sample number of combinations or restorations that have (more than 3), while found that (76) of the study sample, representing a rate of (25.3%) of the total study sample number of combinations or restorations that have (one restoration ), while it was found that (74) of the study sample, representing a rate of (24.7%) of the total study sample number of combinations or restorations that have (two restorations), and finally found that (32) of the study sample, representing a rate of ( 10.7% ) of the total study sample number of combinations or restorations that they have (three restorations).
Table 4: Distribution of the study sample according to the number of restorations.
| No. of FPD and Restorations | Sample size (n) | Percentage |
|---|---|---|
| 1 | 76 | 25.3% |
| 2 | 74 | 24.7% |
| 3 | 32 | 10.7% |
| More than 3 | 118 | 39.3% |
| Total | 300 | 100% |
From Table 5, it is indicated that the (124) of the study sample, representing a rate of (41.3%) of the total members of the duration where treatment combinations or restorations (over a year), while it was found that (73) of the study sample, representing a rate of (24.3%) of the total study sample duration where treatment combinations or restorations (before 6 months), while it was found that (52) of the study sample, representing a rate of (17.3%) of the total study sample wares or restorations (a month ago) and, finally, it was found that (51) of the study sample, representing a rate of (17%) of the total study sample duration where treatment combinations or restorations (a year ago).
Table 5: Time of dental treatment.
| Time of completion of the treatment of FPD or Restorations? | Sample size (n) | Percentage |
|---|---|---|
| Before month | 52 | 17.3% |
| Before 6 months | 73 | 24.3% |
| Before a year | 51 | 17.0% |
| More than this | 124 | 41.3% |
| Total | 300 | 100% |
Through a review of Table 6 shows that the 194) of the study sample, representing a rate of (64.7%) of the total members were subjected to treatment (restorations), while it was found that (53) of the study sample, representing a rate of (17.7%) of the total members of the sample The study underwent treatment (fixtures and restorations together), while it was found that (32) of the study sample, representing a rate of (10.7%) of the total study sample were subjected to treatment (formulations), and finally found that (11) of the study sample, representing a rate of (3.7%) of the total study sample were subjected to treatment (formulations, fillers, implant) and finally found that (10) of the study sample, representing a rate of (3.3%) of the total study sample were subjected to treatment (Implant).
Table 6: Type of dental treatment.
| What is the type of treatment you have? | Sample size (n) | Percentage |
|---|---|---|
| FPD | 32 | 10.7% |
| Restorations | 194 | 64.7% |
| Implant | 10 | 3.3% |
| All of them | 11 | 3.7% |
| FPD and Restorations | 53 | 17.7% |
| Total | 300 | 100% |
Through a review of the Table 7 shows that the vast majority (179) of the study sample, representing a rate of (59.7%) do not suspect any of the conditions listed above, while it was found that (46) of the study sample, representing a rate of (15.3%) of the total members of the sample the study complained of (psychological stress), while it was found that (28) of the study sample, representing a rate of (9.3%) of the total study sample complain (arthritis), while it was found that (21) of the study sample, representing a rate of (7%) of the total study sample complain (musculoskeletal disorders), also found that (17) of the study sample, representing a rate of (5.7%) of the total study sample complain (neurological disorders), and finally equal proportion of the study sample who complain of (psychological pressure and neurological disorders, psychological pressure and muscle and nerve disorders).
Table 7: Patients suffer of other diseases.
| Do you suffer of any of the following diseases? | Sample size (n) | Percentage |
|---|---|---|
| Neurological disorders | 17 | 5.7% |
| Muscular disorders | 21 | 7.0% |
| Arthritis | 28 | 9.3% |
| Psychological pressure | 46 | 15.3% |
| Psychological pressure and neurological disorders | 1 | .3% |
| Psychological pressure and muscle and nerve disorders | 1 | .3% |
| Psychological pressure and arthritis | 7 | 2.3% |
| I am not suffering from any of the above diseases | 179 | 59.7% |
| Total | 300 | 100% |
Can be seen from Table 8 that the (151) of the study sample, representing a rate of (50.3%) complain (dental caries), while it was found that (29) of the study sample, representing a rate of (9.7%) of the total study sample complain (dental caries and teeth fracture), while it was found that (20) of the study sample, representing a rate of (6.7%) of the total study sample complain (caries in teeth and an imbalance in the match), while it was found that (12) of the study sample representing (4%) of the total study sample complain (break-up teeth), also found that (11) of the study sample, representing a rate of (3.7%) of the total study sample complain of (problems in the fixtures and a defect in the match), and found also that (9) of the study sample, representing a rate of (3%) of the total study sample complain of (a defect in the match), while it was found that (5) of the study sample, representing a rate of (1.7%) of the total study sample complain of decay in teeth and problems in formulations, and finally found that (4) of the study sample, representing a rate of (1.3%) of the total study sample members complain of (problems in the formulations).
Table 8: Suffering from other teeth problem.
| Do you suffer from any of the following problems in teeth | Sample size (n) | Percentage |
|---|---|---|
| Dental caries | 151 | 50.3% |
| Teeth fracture | 12 | 4.0% |
| Occlusion | 9 | 3.0% |
| Problems in FPD | 4 | 1.3% |
| Teeth caries and problems in FPD | 5 | 1.7% |
| Dental caries and Teeth fracture | 29 | 9.7% |
| Dental caries and Occlusion | 20 | 6.7% |
| Problems in FPD and Occlusion | 11 | 3.7% |
| Nothing at all | 59 | 19.7% |
| Total | 300 | 100% |
Seen from Table 9 that the (117) of the study sample, representing a rate of (39%) of the total study sample complain of the presence of caries in teeth, while it was found that (105) of the study sample, representing a rate of (35%) of the total members the study sample does not complain of anything, while it was found that (28) of the study sample, representing a rate of (9.3%) of the total study sample complain (break in fixtures or restorations).
Also, it was found that (19) of the study sample representing a rate of (6.3%) of the total study sample complain of (the presence of caries in teeth and break in fixtures or restorations), while equal proportion of the study sample who suffer from (a rise in installations) with the proportion of the study sample who suffer from (decrease of the level of congruence) with a rate of (3.7%) of the total study sample for both of them, and found that (6) of the study sample, representing a rate of (2%) of the total study sample complain of (the existence of decay and a rise in installations).
Finally, we found that (3) of the total study sample, representing a rate of (1%) of the total study sample members complain of (the existence of decay in the teeth and lower the level of capability
Table 9: Complaining from any problems in FPD or Restorations.
| Do you complain from any of the following problems in FPD or Restorations | Sample size (n) | Percentage |
|---|---|---|
| Dental caries | 117 | 39.0% |
| FPD or Restorations Fracture | 28 | 9.3% |
| High occlusion in FPD | 11 | 3.7% |
| Low occlusion in FPD | 11 | 3.7% |
| Dental caries and teeth fracture in FPD or Restoration | 19 | 6.3% |
| Dental caries and high occlusion in FPD | 6 | 2.0% |
| Dental caries and low occlusion in FPD | 3 | 1.0% |
| Nothing at all | 105 | 35.0% |
| Total | 300 | 100% |
From Table 10 and Figure 1 , it is indicated that (71.3%) of the total study sample did not feel any problem when undergoing treatment combinations, while it was found that (16.7%) of the study sample are problems when undergoing treatment for restorations, and finally found that (12%) of the study sample are sometimes problems when undergoing treatment combinations. Also (68.3%) of the total study sample does not match the teeth feel change upon completion of the treatment, while it was found that (20.7%) of the study sample are changing the match dental Upon completion of the treatment.
Table 10: Diagnostic questions for TMD.
| No. | Diagnostic questions | Freq. and percentage | Agreement degree | Mean | SD | Chi-Square | p.value | ||
|---|---|---|---|---|---|---|---|---|---|
| Sometimes | No | Yes | |||||||
| 1 | Did you feel any problem when having FPD? | Freq. | 36 | 214 | 50 | 2.0467 | 0.53427 | 195.92 | 0.000 |
| % | 12% | 71.3% | 16.7% | ||||||
| 2 | Did you feel change in teeth after treatment? | Freq. | 33 | 205 | 62 | 2.0967 | 0.55529 | 169.58 | 0.000 |
| % | 11% | 68.3% | 20.7% | ||||||
| 3 | Did you face difficulty in opening mouth? | Freq. | 34 | 243 | 23 | 1.9633 | 0.43507 | 307.34 | 0.000 |
| % | 11.3% | 81% | 7.7% | ||||||
| 4 | Did you face difficulty in moving the mandible from one side to another? | Freq. | 48 | 231 | 21 | 1.91 | 0.47185 | 261.06 | 0.000 |
| % | 16% | 77% | 7% | ||||||
| 5 | Do you feel pain in muscles when chewing? | Freq. | 54 | 214 | 32 | 1.9267 | 0.53125 | 197.36 | 0.000 |
| % | 18% | 71.3% | 10.7% | ||||||
| 6 | Do you feel pain in ear and neck regions? | Freq. | 34 | 232 | 34 | 2 | 0.47689 | 261.36 | 0.000 |
| % | 11.3% | 77.3% | 11.3% | ||||||
| 7 | Do you feel clicking in TMJ when chewing? | Freq. | 51 | 190 | 59 | 2.0267 | 0.60595 | 121.82 | 0.000 |
| % | 17% | 63.3% | 19.7% | ||||||
| 8 | Do you grind teeth during sleeping? | Freq. | 29 | 247 | 24 | 1.9833 | 0.42069 | 324.26 | 0.000 |
| % | 9.7% | 82.3% | 8% | ||||||
| 9 | Do you feel inclination of jaw when opening it? | Freq. | 22 | 249 | 29 | 2.0233 | 0.41234 | 333.26 | 0.000 |
| % | 7.3% | 83% | 9.7% | ||||||
| 10 | Do you finddifficultieswhen you openor closethe mouth | Freq. | 44 | 238 | 18 | 1.9133 | 0.44701 | 289.04 | 0.000 |
| % | 14.7% | 79.3% | 6% | ||||||
| 11 | Do you have problem with matching? | Freq. | 18 | 240 | 42 | 2.08 | 0.44074 | 296.88 | 0.000 |
| % | 6% | 80% | 14% | ||||||
| 12 | Do you feel FPD or restorations had affected the jaw? | Freq. | 31 | 231 | 38 | 2.0233 | 0.47982 | 257.66 | 0.000 |
| % | 10.3% | 77% | 12.7% | ||||||
| 13 | Did you visit dentist to explain your problem? | Freq. | 17 | 225 | 58 | 2.1367 | 0.48176 | 242.78 | 0.000 |
| % | 5.7% | 75% | 19.3% | ||||||
| 14 | Did you usedrestorations to hinder teeth grinding? | Freq. | 11 | 273 | 16 | 2.0167 | 0.30004 | 449.06 | 0.000 |
| % | 3.7% | 91% | 5.3% | ||||||
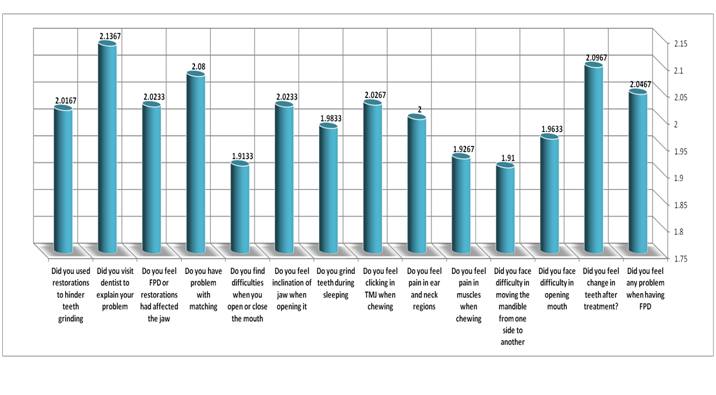
Figure 1: Means of diagnostic questions.
While it was found that (11%) of the study sample feel sometimes changing the match teeth upon completion of treatment. (81%) of the total study sample do not face difficulty in opening their mouth when installation or fillers, while it was found that (11.3%) of the study sample face sometimes difficult to open their mouth when installation or fillers, while found to be (7.7%) of the study sample are having difficulty in opening their mouth when installation or fillers. Also, (77%) of the total study sample do not face difficulty in moving the jaw from side to side when the installation or fillers, while it was found that (16%) of the study sample face sometimes difficult to open their mouth when installation or fillers, while found that (7%) of the study sample are having difficulty in moving the jaw from side to side when the installation or fillers.
Also, (71.3 %) of the total study sample do not feel pain when chewing muscles, while it was found that (18%) of the study sample sometimes feel pain in muscles when chewing, while it was found that (10.7%) of the study sample does not feel pain in muscles when chewing. Also (77.3 %) of the total study sample did not feel pain in the ear or tenderness, while it was found that (11.3%) of the study sample sometimes feel pain in the ear or tenderness, also found that (11.3%) of the sample the study experienced pain in the ear or tenderness. Also, (63.3 %) of the total study sample did not feel jaw hinge when you open or when chewing, while it was found that (19.7% ) of the study sample feel jaw hinge when you open or when chewing, while it was found that (17%) of the study sample feel sometimes jaw hinge when you open or when chewing. Also, (82.3 %) of the total study sample does not grind their teeth at bedtime, while it was found that (9.7%) of the study sample in a few cases, grind their teeth at bedtime, while it was found that (8%) of the study sample grind their teeth at bedtime
Moreover, (83%) of the total study sample did not feel Milan jaw when you open or close towards any destination, while it was found that (9.7%) of the study sample feel Milan jaw when you open or close towards any destination, while it was found that (7.3%) the study sample of individuals sometimes feel Milan jaw when you open or close towards any party and (79.3%) of the total study sample do not find difficulties when you open or close the mouth, while it was found that (14.7%) of the study sample have sometimes difficulties when you open or close the mouth, while it was found that (7.3%) of the sample the study sometimes feel Milan jaw when you open or close towards any party. And (80%) of the total study sample have a problem when the match in hand without the other, while it was found that (14%) of the study sample have a problem when the match in hand without the other.
Furthermore, it was found that (6%) of the study sample find sometimes a problem when the match in hand without the other and (77%) of the total study sample did not believe that the treatment of wares or restorations impact on the jaw, while it was found that (12.7%) of the study sample believe that the treatment of wares or restorations, while it was found that (10.3%) of individuals in the study sample sometimes think that the treatment of wares or restorations impact on the jaw and (75%) of the total study sample have not visited the Dentist to explain to him the problem that suffer from it, while it was found that (19.3%) of the study sample had visited the Dentist to explain to him the problem that they have, while it was found that (5.7% ) of the study sample who sometimes visit the dentist to explain to him the problem which they suffer. And (91%) of the total study sample did not use the combination to prevent grinding the teeth during sleep, while it was found that (5.3% ) of the study sample used the combination to prevent grinding the teeth during sleep, while it was found that (3.7%) of the study sample in some often use the combination to prevent teeth grinding during sleep.
Seen from table 11 include the following: A positive relationship between the wave (TMD) and variable age as the value of the relationship (0.153). The existence of an inverse relationship between (TMD) and both (number of combinations or restorations, the time to complete treatment combinations or restorations, the type of treatment, you suffer from the following diseases, you complain about any of the following problems in the teeth, do you complain about any of the following problems in the FPD or restorations), reaching values of the relationship (-0.77, -0.130, -0.151, -0.97, -0.66, -0.121)
Table 11: Relationship between TMD and other variables.
| Do you feel problem in FPD or restorations | Do you suffer from the following problems | Do you suffer from the following diseases | Treatment problem | Time of completing FPD or restorations | No. of FPD or restorations | Age | Relation |
|---|---|---|---|---|---|---|---|
| -0.121 | -0.66 | -0.97 | -0.151** | -0.130* | -0.77 | 0.153** | TMD |
Discussion
Our research was focused to find a relationship of TMD with FPD and restorative treatment in Riyadh city. Data collection was carried out by means of a self-applied questionnaire. The etiology of TMD has been considered to be one of the most controversial issues in clinical dentistry. A majority of dental practitioners believe that occlusal disturbances can cause or are closely related to TMD, and many therefore also include occlusal adjustment as an initial treatment for TMD, whereas most TMD experts hold opposing views[4-6].
Few studies have been reported on the prevalence of TMD in Saudi Arabia in normal permanent dentition and adults[8,9]. Restorative procedures are divided into two types-(1) Operative and (2) fixed prosthodontic. Operative procedures are those in which the final restorations are fabricated intrao-rally (e.g., an amalgam, a composite resin). Fixed prosthodontic procedures are those that involve extraoral fabrication with final adjustment and cementation in the mouth (e.g., inlays, onlays , full crowns, fixed partial dentures[7].
n our research result we found that there is direct relationship between TMD & age of patients representing rate of (0.153), This value are in agreement with the previous study[17], this investigation revealed that radiographic appearance of TMJ varied widely, remodeling changes were commonly seen, and there was no direct linear relationship between age and radiographic changes in condylar morphology. Also, we found there is reverse relation between TMD with Restorations and FPD numbers representing rate of (-0.77) this agree with” Undergo corrective dental treatments. Corrective treatments including replacing missing teeth and using crowns, bridges, or braces to balance the biting surfaces of your teeth or to correct a bite problem” (23). And there is reverse relation between TMD with time of completing FPD &restorative treatment (-0.13) cause of a major of our sample doesn’t suffer from TMD problem
TMD relation with other diseases (-0.97) cause of 98% of our sample didn’t complain of medical problem. Because many other conditions can cause similar symptoms to TMD –including toothache, sinus problems, arthritis, or gum disease – your dentist will conduct a careful patient history and physical examination to determine the cause of your symptoms[18].
Conclusion
This research discusses and reviews correlation of TMD with FPD and restorative treatment, including role of FPD, restorative treatment and many factors in TMD. Causes of TMD are not clear, but dentists believe that symptoms arise from problems with the muscles of the jaw or with the parts of the joint itself. Carefully, observed patient history and physical examination to determine the cause of TMD symptoms. It still need more and more research to clarify this problem, its causes in Saudi Arabia. Also, should be community awareness of TMD problem and its symptoms and signs.
Acknowledgement:
Thanks Prof. Magdy Hamam for his efforts and guidance in our research.
References
- 1. De Boever, J.A., Carlsson, G.E., Klineberg, I.J. Need for occlusal therapy and prosthodontic treatment in the management of temporomandibular disorders. Part I. Occlusal interferences and occlusal adjustment. (2000) J Oral Rehabil 27(5): 367-379.
- 2. De Boever, J.A., Carlsson, G.E., Klineberg, I.J. Need for occlusal therapy and prosthodontic treatment in the management of temporomandibular disorders. (2000) Journal of Oral Rehabilitation 27(8): 647-659.
- 3. Laskin, D., Gale, E. The President’s Conference on the Examination, Diagnosis and Management of Temporomandibular Disorders. (1982) American Dental Association Chicago.
- 4. LeResche, L., Saunders, K., Von Korff, M.R., et al. Barlow, and S.F. Dworkin, Use of exogenous hormones and risk of temporomandibular disorder pain. (1997) Pain 69(1-2): 153-160.
- 5. Glaros, A.C., Glass, E.G., McLaughlin, L. Knowledge and beliefs of dentists regarding temporomandibular disorders and chronic pain. (1994) Journal of oro facial pain 8(2): 216-222.
- 6. Arbree, N.S., Campbell, S.D., Renner, R.P., et al. A survey of temporomandibular disorder conducted by the Greater New York Academy of Prosthodontics. (1995) J Prosthet Dent 74(5): 512-516.
- 7. Okeson, J.P. Management of temporomandibular disorders and occlusion. (2014) Elsevier Health Sciences.
- 8. Farsi, N.M.A. Symptoms and signs of temporomandibular disorders and oral parafunctions among Saudi children. (2003) Journal of oral rehabilitation 30(12): 1200-1208.
- 9. Jagger, R.G., Wood. C. Signs and symptoms of temporomandibular joint dysfunction in a Saudi Arabian population. (1992) Journal of oral rehabilitation 19(4): 353-359.
- 10. Okeson, J.P. Orofacial pain: guidelines for assessment, diagnosis, and management. (1996) Quintessence Publishing.
- 11. Zarb, G., Bolender, C., Carlsson, G. Single complete dentures opposing natural or restored teeth: Boucher’s prosthodontic treatment for edentulous patients; 11th edn. (1997) Mosby St. Louis Missouri 418.
- 12. Gazit, E., Fitzig, S., Lieberman, M.A. Reproducibility of occlusal marking techniques. (1986) J Prosthet Dent 55(4): 505-509.
- 13. Takai, A., Nakano, M., Bando, E., et al. Influence of occlusal force and mandibular position on tooth contacts in lateral excursive movements. (1995) The Journal of prosthetic dentistry 73(1): 44-48.
- 14. Hellsing, G. Occlusal adjustment and occlusal stability. (1988) The Journal of prosthetic dentistry 59(6): 696-702.
- 15. Clark, G.T. Etiologic theory and the prevention of temporomandibular disorders. (1991) Adv Dent Res 5(1): 60-66.
- 16. Tsukiyama, Y., Baba, K., Clark, G.T. An evidence-based assessment of occlusal adjustment as a treatment for temporomandibular disorders. (2001) The Journal of prosthetic dentistry 86(1): 57-66.
- 17. Mathew, A.L., Sholapurkar, A.A., Pai, K.M. Condylar changes and its association with age, TMD, and dentition status: a cross-sectional study. (2011) International journal of dentistry.
- 18. Temporomandibular Joint Disorders (TMD, TMJ).










