
Diagnosis, Prognosis and Management of Incidental Metastatic Melanoma to Breast, Axilla and Regional Lymph Nodes in a Ninety-Year-Old Female
Quan Nguyen*, Nita Kommula, Angelica Robinson, Safaraz Sadruddin, Anne Lee, David Pacheco, Shadan Alwan, Taylor Harmon, Audrey Albach, Sara Ortiz, Suimin Qiu, Sandra Hatch
Affiliation
Department of Radiology, UTMB, Texas, USA
Corresponding Author
Quan Nguyen, Department of Radiology, UTMB, Texas, USA; E-mail: qunguyen@utmb.edu
Citation
Nguyen, Q., et al. Diagnosis, Prognosis and Management of Incidental Metastatic Melanoma to Breast, Axilla, and Regional Lymph Nodes in a Ninety-Year-Old Female. (2018) Int J Cancer Oncol 5(2): 64- 67
Copy rights
© 2018 Nguyen, Q. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Abstract
Malignant melanoma arises from melanocytic cells in the skin and mucosal membranes. Malignant melanomas predominantly develop in areas that are exposed to sunlight including the face, back, or extremities. Because melanoma predominantly occurs in the skin and mucous membranes, malignant melanoma of the breast is particularly rare. The incidence of primary melanoma of the breast is < 5% of all melanomas[1]. Furthermore, secondary tumors of the breast from metastatic malignancies are quite uncommon. Of metastatic malignancies to the breast, melanoma is, however, among the most common[2]. Therefore, metastasis to the breast must be considered in any patient with a known primary malignant tumor history who presents with a breast mass. A full diagnostic work up with observation of the clinical pathological features, immunohistochemical staining methods and tissue origin are required to distinguish primary malignant melanoma of the breast from possible metastatic melanoma.
Introduction
Case Report
Our case details the course of a 90 year old female with a past medical history of hypertension, arthritis, and invasive melanoma of the back which was treated with surgical resection “several years” prior. She was evaluated in the emergency department after being found unconscious in her home. During intake history and physical, a large right breast mass was appreciated. The patient was aware of the mass which had been progressively increasing in size for 2 - 3 years. She elected not to seek treatment due to social circumstances. Functional status assessment revealed a patient that lives alone, has neighbors that occasionally check on her, and ambulates with cane and walker. At initial presentation a CT of the thorax (Figure 1) revealed multiple right breast masses in addition to multiple enlarged and necrotic right axillary and supraclavicular lymph nodes. Primary breast malignancy was raised a concern and follow up breast consultation and biopsy was recommended.
During her inpatient stay, the patient underwent diagnostic work up for her breast mass in the breast imaging department. Diagnostic mammogram (Figure 2) showed a normal left breast. However, given the right breast was enlarged and deformed by internal masses, it was not amenable to diagnostic mammogram. Targeted ultrasound (Figure 3) of the right breast revealed a conglomerate of masses at 11 o’clock, approximately 17 cm from the nipple. Axillary, supraclavicular, and infraclavicular lymphadenopathy was also observed. These findings warranted a BI-RADS category of 5, highly suggestive of malignancy, and the patient subsequently underwent core biopsy (Figure 4) of the conglomerate of masses.
The morphological findings and immunohistochemical staining profile (Figure 6 - 10) of the biopsy sections showed high grade malignant neoplastic cells with melanin pigment (Figure 5), suggestive of recurrent melanoma and highly suspicious for advanced metastatic disease.
The patient was given an appointment with a breast surgeon. However, she was recommended palliative care and oncologic surveillance as she was not a suitable candidate for immunotherapy, the standard of care, due to consistently poor performance status with ongoing acute issues.
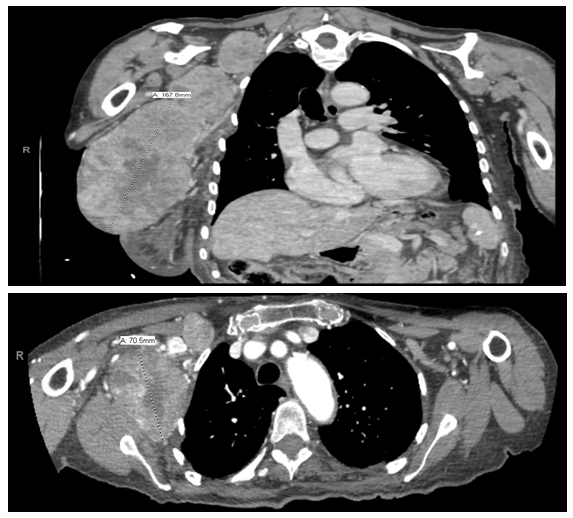
Figure 1: Initial CT Thorax obtained in the ER shows multiple enhancing right breast masses and conglomerates of supraclavicular lymph nodes, highly concerning for malignancy. Biopsy was recommended.
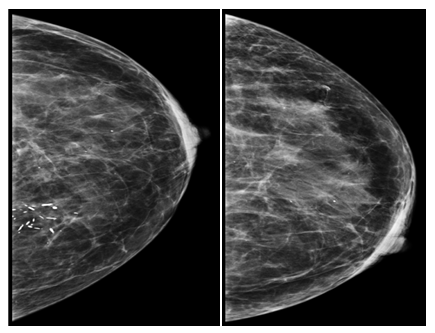
Figure 2: Diagnostic Left Breast Mammogram.
Left Breast Findings: Negative. Secretory calcifications incidentally noted in the medial breast posteriorly. The right breast was not amenable to mammography.
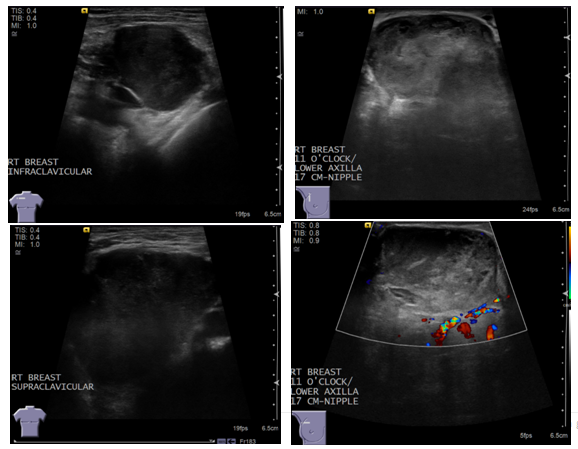
Figure 3: Diagnostic Right Breast Ultrasound.
Right Breast Findings: Targeted ultrasound of the right breast revealed conglomerates of masses in the breast and low axilla as well as supraclavicular and infraclavicular lymphadenopathy. However, given the large size of the mass which was beyond the confines of the ultrasound transducer probe, the measurements were unreliable. These findings were assigned a BI-RADS category of 5, highly suggestive of malignancy. Ultrasound-guided core biopsy was recommended.
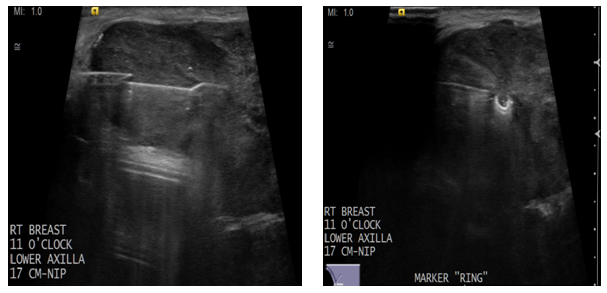
Figure 4: Ultrasound Guided Biopsy 11/27/2017.
Ultrasound guided biopsy and micromarker placement through a large mass in the right breast.
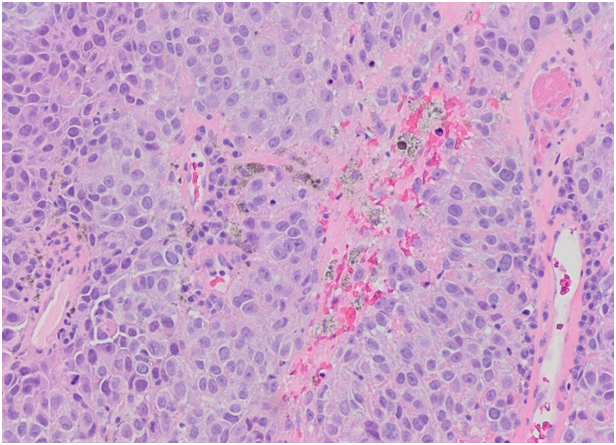
Figure 5: H&E, 10x magnification. Breast, right, 11 o’clock lower axilla, 17 cm from nipple, core biopsy: Sections show high-grade malignant neoplastic cells with melanin pigment. Abundant mitotic figures and focal necrosis are noted.
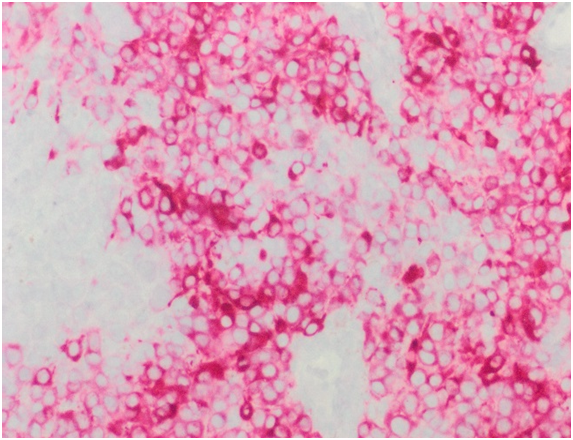
Figure 6: MART1/Melan-A IHC stain using a red chromogen shows strong positivity in the melanoma cells.
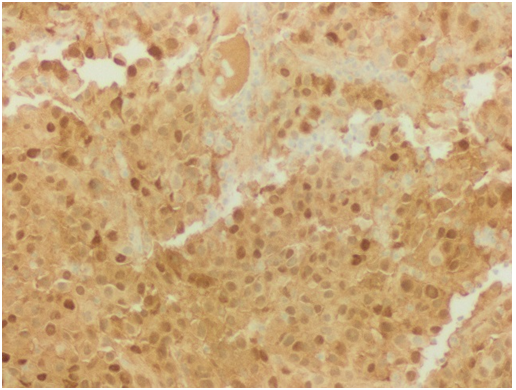
Figure 7: S100 showing strong and diffuse nuclear and cytoplasmic positivity in melanoma cells.
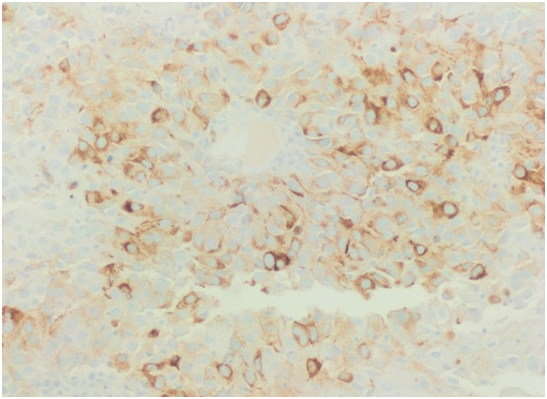
Figure 8: HMB45 showing cytoplasmic positivity in melanoma cells.
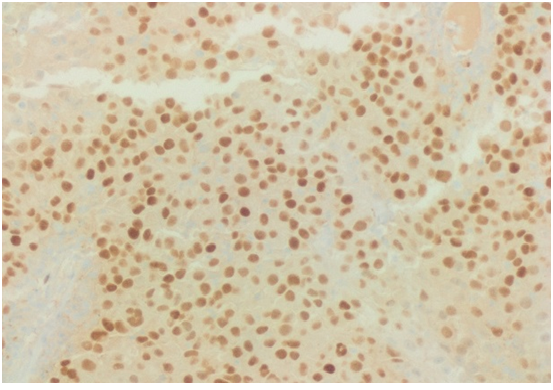
Figure 9: SOX10 shows diffuse nuclear staining in melanoma cells.
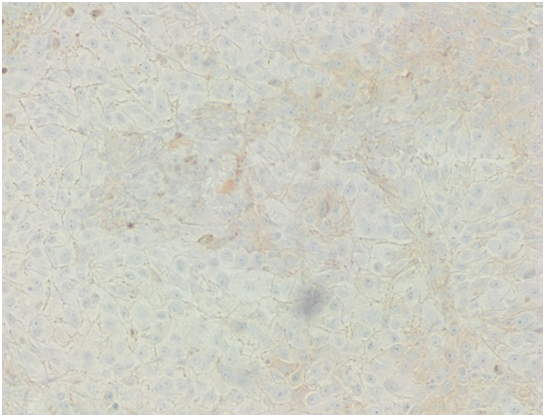
Figure 10: GATA3, a breast carcinoma marker, is negative in the melanoma cells.
Discussion
The four main types of melanoma are superficial spreading melanoma (most common type), nodular melanoma (second most common type), lentigo maligna melanoma (less common), and acral lentiginous melanoma (rarest type)[1]. The superficial spreading melanoma subtype usually manifests with the classic early signs of melanoma (ABCDEs). The hallmark of nodular melanoma is rapid growth. Lentigo maligna occurs on sun-damaged atrophic skin in elderly persons, usually in the seventh and eighth decades of life. Development of acral lentiginous melanoma does not seem to be associated with sun exposure. The stage and tumor features of our patient’s original melanoma were unavailable to the team at presentation.
Metastatic melanoma of unknown primary can arise in lymph nodes, distant organs, or both[2]. Unknown primary site represents up to 20 % of metastatic melanomas, depending on the series[3]. The prognosis of melanoma of unknown primary, when adjusted for stage at presentation of metastatic disease, appears to better than melanoma of known primary site[4].
Management of metastatic melanoma differs for younger patients with good functional status versus elderly patients with poor functional status. Functional status is a surrogate for activities of daily living. Per review of the National Comprehensive Cancer Network Guidelines Version 2.2017, the presently available data regarding radiation and surgery for melanoma in older adults suggest that no specific age-related recommendations can be made. Upon oncology consult, our 90 year old patient was recommended palliative care and oncologic surveillance as patient was unlikely to be a candidate for immunotherapy (standard of care for a melanoma diagnosis) and had a consistently poor performance status with ongoing acute issues.
Older age is recognized as an independent poor prognostic factor for melanoma based on analysis of large single-institutional and multi-institutional databases of cutaneous melanoma patients[5]. The most striking differences in melanoma incidence and mortality occur in individuals over age 65, although modest differences in age-specific incidence and mortality are notable in those over age 50[6]. Early detection and screening to reduce melanoma mortality are crucial in older individuals who are both more likely to acquire and to die from melanoma. Reasons for differences in prognosis in older patients have been attributed to a diminished immune response with increased age[7,8], changes in host immune biology[9], decreased ability to repair DNA in sun-damaged melanocytes[8], under treatment with increasing age (narrower surgical margins, fewer staging procedures due to other medical conditions)[10].
Treatment options in the elderly are limited due to decreased inability to tolerate medication side effects or toxicity, comorbid medical conditions, increased likelihood of drug interactions, and potential exclusion from clinical trials based on age eligibility criteria. Medical comorbidities that accumulate with increasing age may limit therapy with antineoplastic agents, and particularly with the biologic agents known as cytokines and interferons. Patients older than 70 years or of diminished performance status were excluded from many of the original trials of biologic antitumor agents in melanoma. Patients who have underlying lung dysfunction and diminished diffusing capacity of the lung for carbon monoxide (DLCO), or limitations of cardiac function with congestive failure or angina have been excluded from interleukin [IL]-2, Proleukin treatment due to toxicities of fever and capillary leak syndrome[5,6]. The main drawback of biologic agents is induction of a flu-like syndrome which can be lethal in the elderly, who may have underlying organic syndromes or live alone[11].
The benefit of available treatments for elderly patients with metastatic is uncertain because most of the patients studied in clinical trials are younger in age. After melanoma was discovered to be an immunogenic tumor, biologic agents, such as interleukin (IL)-2 and interferon-α, have been routinely used in selected patients individually or combined with chemotherapeutic agents[12]. Biochemotherapy has not undergone systematic testing in the elderly population because of toxicity concerns and because elderly patients are difficult to accumulate in clinical trials due to their underlying comorbidities and inability to travel to centers conducting studies[13].
References
- 1. Tung, R.., Vidimos, A. Melanoma. (2010) Cleveland Clinic Center for Continuing Education.
PubMed||CrossRef||Others
- 2. Kibbi, N., Kluger, H., Choi, J.N. Melanoma: Clinical Presentations. In: Kaufman H., Mehnert J. (eds) Melanoma. (2016) Cancer Treat Res, Springer 167: 107-129.
PubMed||CrossRef||Others
- 3. Lee, C.C., Faries, M.B., Wanek, L.A., et al. Improved survival for stage IV melanoma from an unknown primary site. (2009) J Clin Oncol 27(21): 3489–3495.
- 4. Lee, C.C., Faries, M.B, Wanek, L.A., et al. Improved survival after lymphadenectomy for nodal metastasis from an unknown primary melanoma. (2008) J Clin Oncol 26(4): 535–541.
- 5. Russo, A.E., Ferraù, F., Antonelli, G., et al. Malignant melanoma in elderly patients: biological, surgical and medical issues. (2015) Expert Rev Anticancer Ther 15(1): 101-108.
- 6. Susan, M., Swetter, M.D., Alan, C., et al. Melanoma in the Older Person. (2004) Oncol J 18(9).
PubMed||CrossRef||Others
- 7. Walford, R.L. Immunology and aging. (1980) Am J Clin Pathol 74(3): 247-253.
- 8. Morris, B.T., Sober, A.J. Cutaneous malignant melanoma in the older patient. (1986) Dermatol Clin 4(3): 473-480.
PubMed||CrossRef||Others
- 9. Loggie, B., Salve, G.R., Bean, J., et al. Invasive cutaneous melanoma in elderly patients. (1991) Arch Dermatol 127: 1188-1193.
- 10. Levine, J., Kopf, A.W., Rigel, D.S., et al. Correlation of thicknesses of superficial spreading malignant melanomas and age of patients. (1981) J Dermatol Surg Oncol 7(4): 311-316.
- 11. Islam, M., Frye, R.F., Richards, T.J., et al. Differential effect of IFNalpha-2b on the cytochrome P450 enzyme system: A potential basis of IFN toxicity and its modulation by other drugs. (2002) Clin Cancer Res 8(8): 2480-2487.
- 12. Legha, S.S., Ring, S., Bedikian, A., et al. Treatment of metastatic melanoma with combined chemotherapy containing cisplatin, vinblastine, dacarbazine (CVD) and biotherapy using interleukin-2 and interferon alpha. (1996) Ann Oncol 7(8): 827-835
PubMed||CrossRef||Others
- 13. Hegde, U.P., Grant-Kels, J.M. Metastatic melanoma in the older patient: Special considerations. (2013) Clin Dermatol 31(3): 311-316.










