
Double Philadelphia Chromosome-Positive B Acute Lymphoblastic Leukemia
Honggang Cao, Jing Li, Tao Wu*, Dongfeng Mao, Cunbang Wang, Hai Bai
Affiliation
Department of Hematology, Lanzhou General Hospital, Lanzhou Command, Lanzhou, Gansu, China
Corresponding Author
Dr. Tao Wu, Department of Hematology, Lanzhou General Hospital, Lanzhou Command, 333 South Binhe Rd, Lanzhou, Gansu, 730050, China,Tel: +86-13919939297/ Fax: +86-931-2665486; E-mail:wutao2009@126.com
Citation
Wu, T., et al. Double Philadelphia Chromosome-Positive B Acute Lymphoblastic Leukemia. (2018) Int J Hematol Ther 4(1): 34- 35.
Copy rights
© 2018 Wu, T. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Introduction
Philadelphia (Ph) chromosome is the derivative chromosome 22 that results from reciprocal translocation t(9;22) (q34;q11). It has been found in about 95% of chronic myeloid leukemia (CML), less often presented in acute lymphocytic leukemia (ALL, about 25% in adult and 2 - 4% in pediatrics) and occasionally observed in acute myelogenous leukemia (AML)[1]. While double Ph chromosomes can be reported in some cases of CML during blastcrisis, it is rarely reported in ALL. We present a rare case of a lady with a diagnosis of double Ph-positive B-ALL who achieved a continuous complete response after treatment with a combination of conventional chemotherapy and tyrosine kinase inhibitor (TKI) as follows.
Case Report
A 53-year-old lady was admitted to our hospital with half a month history of fever, fatigue and dizziness. Physical examination revealed palpable sternal tenderness. Peripheral blood tests showed white cell count 95.39 × 109/L, hemoglobin 100 g/L and platelet 18 × 109/L. Peripheral blood cell morphology showed: lymphoblasts 44%, immature lymphocytes 50%. Bone marrow cytology showed 98% blasts which were heterogeneous in size. Immunophenotype of the blast cells showed: CD10+, CD13+, CD19+, CD20+, CD22+, CD33+, CD34+. Chromosome analysis revealed a 47 ~ 50, XX, +5, +8, t(9;22) (q34;q11), + der(22) t (9;22) karyotype (Figure 1). In conclusion, her final diagnosis was B-ALL with double Ph chromosome. She was initially treated with conventional chemotherapy and regular intrathecal chemotherapy. As Ph chromosome was positive, imatinib was subsequently administered. She achieved a complete remission and had stayed in continuous remission for two months.
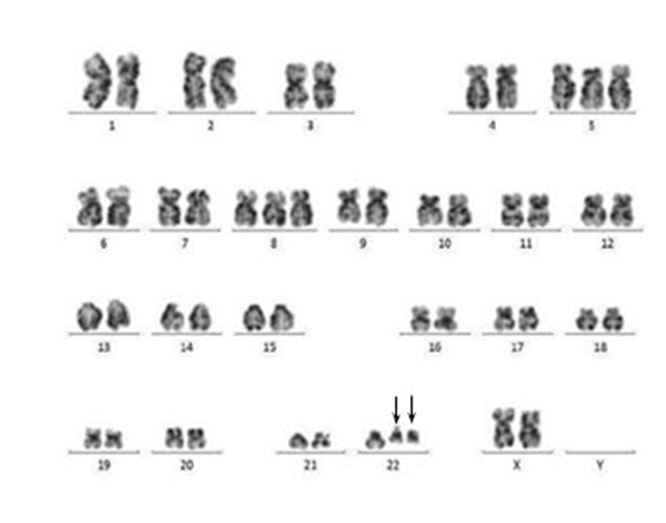
Figure 1: Karyotype of bone marrow showed 47 ~ 50, XX, +5, +8, t(9;22) (q34;q11), der(22) t(9;22). There was presence of two truncated Ph chromosomes 22 (arrows).
Discussion
Ph chromosome positive ALL is associated with a highly aggressive disease, more resistant to chemotherapy[2], and lower remission rate and shorter survival when compared with Ph chromosomenegative[3]. Affected patients usually present with signs and symptoms related to bone marrow failure. The current standard therapy for Ph chromosome-positive B-ALL ischemotherapy in addition to TKI, and allogeneic stem cell transplantation after first remission is believed to be the treatment of choice in adult Ph chromosome positive ALL, when possible[4].
Double Ph chromosome-positive B-ALL is reported in several case reports worldwide[1,5-7]. The possible mechanism of double Ph chromosome is considered to be the result of non-disjunction occurring during mitosis[1]. However, the clinical significance of double Ph chromosomes in ALL has not been known. It is reported that double Ph chromosome-positive ALL patients have lower probability of complete hematological response, shorter time to progression and inferior overall survival when compared with single Ph chromosome[8].
We describe here the rare case of an elderly female patient with double Ph chromosome-positive B-ALL who stayed in continuous complete remission for two months after initial therapy. As a whole, the case is consistent with the literature reports, but long-term efficacy needs to be further observed. Therefore, a further large number of cases are needed to probe into the clinical significance of double Ph chromosome in B-ALL.
Acknowledgements: This work was sponsored by the grant from the natural science foundation of Gansu Province (145RJZA151).
Authors’ declaration: All authors read and approved the final manuscript. All authors declare no conflict of interest.
References
- 1. Tang, Y.L., Raja Sabudin, R.Z., Leong, C.F., et al. Double Philadelphia chromosome positive B acute lymphoblastic leukemia in an elderly patient. (2015) Malays J Pathol 37(3): 275-279.
- 2. Rowe, J.M., Buck, G., Burnett, A.K., et al. Induction therapy for adults with acute lymphoblastic leukemia: results of more than 1500 patients from the international ALL trial: MRC UKALL XII/ECOG E2993. (2005) Blood 106(12): 3760-3767.
- 3. Secker-Walker, L.M., Craig, J.M., Hawkins, J.M., et al. Philadelphia positive acute lymphoblastic leukemia in adults: age distribution, BCR break - point and prognostic significance. (1991) Leukemia 5(3): 196-199.
PubMed||CrossRef||Others
- 4. Ottmann, O.G., Wassmann, B. Treatment of Philadelphia chromosome–positive acute lymphoblastic leukemia. (2005) ASH Education Book 2005(1): 118-122.
PubMed||CrossRef||Others
- 5. Vaz de Campos, M.G., Chauffaille, M.L.L.F., Rodrigues, C.A., et al. A rare case of Acute Lymphocytic Leukemia (ALL) presenting with double Philadelphia chromosome - relapse or secondary leukemia? (2003) Genet Mol Biol 26(3): 249-251.
PubMed||CrossRef||Others
- 6. Takasaki, H., Kanamori, H., Takabayashi, M., et al. Double Philadelphia chromosomes positive acute lymphocytic leukemia. (2003) Leuk Lymphoma 44(4): 735–736.
- 7. Yahata, N., Tauchi, T., Kimura, Y., et al. Double Philadelphia chromosomes in acute lymphocytic leukemia. (2000) Cancer Genet Cytogenet 121(1): 101–102.
- 8. Wassmann, B., Pfeifer, H., Scheuring, U.J., et al. Early prediction of response in patients with relapsed or refractory Philadelphia chromosome-positive acute lymphoblastic leukemia (Ph+ALL) treated with imatinib. (2004) Blood 103(4): 1495-1498.










