
First trimester fetal biparietal diameter and head circumference in Chinese population
Min CHEN1,2,3,4,5,6#*, Xin YANG7#, Qizhen ZHENG1,2,3,4, Chun Quan OU8,9, Chin Peng LEE6, Yung Hang LAM10, Mary Hoi Yin TANG6
Affiliation
- 1Department of Fetal Medicine and Prenatal Diagnosis, The Third Affiliated Hospital of Guangzhou Medical University, Guangzhou, 510150, China
- 2Obstetrics & Gynecology Institute of Guangzhou, Guangzhou,510150, China
- 3The Medical Centre for Critical Pregnant Women in Guangzhou, Guangzhou, 510150, China
- 4Key Laboratory for Major Obstetric Diseases of Guangdong Province, Guangzhou, 510150, China
- 5Key Laboratory of Reproduction and Genetics of Guangdong Province
- 6Department of Obstetrics and Gynaecology, The University of Hong Kong, Queen Mary Hospital, Hong Kong, China
- 7Prenatal Diagnosis Center, Guangzhou Maternal and Neonatal Hospital, Guangzhou, 510623, China
- 8Department of Community Medicine, Faculty of Medicine, The University of Hong Kong, Hong Kong, China
- 9Department of Biostatistics, Southern Medical University, Guangzhou, China
- 10Hong Kong Prenatal Diagnosis Center, Hong Kong, China
- ##The two authors contribute equally to this work
Corresponding Author
Min CHEN, Department of Fetal Medicine and Prenatal Diagnosis, The Third Affiliated Hospital of Guangzhou Medical University, Guangzhou, 510150, China, E-mail: edchen99@gmail.com
Citation
Min, C., et al. First Trimester Fetal Biparietal Diameter And Head Circumference In Chinese Population. (2017) J Gynecol Neonatal Biol 3(1): 27-31.
Copy rights
© 2017 Min, C. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Biometry; First trimester; Ultrasound; Fetus; Biparietal diameter; Head circumference
Abstract
Objectives:To establish the reference ranges for fetal biparietal diameter and head circumference obtained by transabdominal ultrasound examination in the first trimester in Chinese women.
Methods:In this prospective cross-sectional study, 1351 normal singleton fetuses were examined transabdominally by 2 experienced observers in the first trimester of pregnancy in which the CRL was between 55 and 84 mm. Measurements of Biparietal Diameter (BPD), head circumference (HC) were prospectively collected. Charts and predictive equations were constructed from data obtained.
Results:Measurements of BPD, HC were correlated with CRL. CRL-based predictive equations were calculated using polynomial least squares regression analysis. HC = 7.710583 + 1.387393 * CRL-0.0037807 * CRL², R² = 0.5735, P = 0.000. BPD = 6.855277 + 0.2389065 * CRL, R² = 0.5355, P = 0.000. CRL-specific biometric charts were constructed.
Conclusions:There was a general increase in fetal biparietal diameter and head circumference with CRL. Chinese fetal biometry might be of help in first-trimester ultrasound examination in the local population.
Introduction
The ultrasound measurement of fetal biometry such as Biparietal Diameter (BPD), Head Circumference (HC), Abdominal Circumference (AC) and Femur Length (FL) are very helpful in detecting fetal abnormalities and intrauterine growth retardation (IUGR). Many studies have established normal charts or curves of fetal biometry[1-3]. But most of these data are based mainly on studies from Western or American populations[1,4]. Leung et al[5] had established fetal biometry charts in Hong Kong Chinese population, but this study was mainly focus on second and third trimester. The aim of this study is to establish reference ranges for fetal biparietal diameter and head circumference between 12 to 14 weeks in a Chinese population.
Materials and Methods
From February 1998 to March 2001, Chinese women seeking prenatal diagnosis for advanced maternal age at 10 – 14 weeks were enrolled into a screening program for structural abnormalities. Pregnancy outcomes were ascertained from the obstetric and neonatal files. The local ethics committee approved the research protocol.
In this cross-sectional study, 1489 singleton fetuses between 12+0 and 14+6 weeks were examined transabdominally by two experienced operators (CPL and YHL). We only included cases with a known normal outcome into the final analysis. Cases with abnormal karyotype and major structural abnormalities, as well as cases of miscarriage or intrauterine death, were excluded. The ultrasound equipment used included the Sequoia with a 6-MHz curvilinear transducer and the Acuson XP 128 with a 5 – 7 MHz curvilinear transducer (Siemens Acuson Inc., Mountain View, CA, USA).
The BPD and HC were measured on a transverse view of the fetal head in a plane showing both thalami and the third ventricle[6,7]. BPD was measured “outer to inner”. HC was measured by placing the ellipse around the outside of the skull bone echoes[8].
The gestational age was ascertained by measurement of fetal crown–rump length (CRL)[9]. Two independent measurements of the BPD and HC were obtained and averaged for the final measurement in the analysis. Intraobserver variability was calculated as described by Bland and Altman[10,11]. The normality of measurements at each week of gestation was assessed using the Kolmogorov–Smirnov test. Mean, the 5th, and 95th centiles of BPD and HC between 11 and 14 weeks of gestation were plotted. Pearson’s correlation was used to analyze the relationship between measurements.
The BPD and HC were analyzed separately as the dependent variable and the gestational age as the independent variable. First, a cubic polynomial (y = a + b × GA + c × GA2 + d × GA3) was fitted. If the cubic coefficient was not significantly different from zero, then a quadratic polynomial was fitted and the same assessment was made of the quadratic coefficient. This process was repeated until no further removal of terms was possible. The equation selected was of the lowest order for which all coefficients of the equation were significantly different from zero, as computed by the full to reduced F test. Regression of the scaled absolute residuals was applied to construct the percentile curves[8,12].
All statistical analysis was performed with SPSS for Windows 18.0 software package (Chicago, IL, USA). A P value of < 0.05 was considered statistically significant. In order to compare our reference equations with two previously published studies[8,13], the means from two published fetal BPD and HC equations were calculated at each week of gestation starting from 12 – 14 weeks. They were then expressed as Z -scores calculated using the formula: Z -score = (XGA − MGA)/SDGA, where XGA was the measured value at a known gestational age, MGA was the mean value obtained with the reference equation used at this gestation, and SDGA was the SD associated with the mean value at this gestation obtained from the reference equation. Results were presented graphically across gestational ages.
Results
In 1351 singleton pregnancies in the final analysis, median maternal age was 37 years (range: 35 – 49 years), median gestational age was 13+4 weeks (range: 12+0 – 14+6 weeks). CRL was between 55 and 84 mm.
The increase in BPD and HC based on the CRL was given by the equation: BPD = 6.855277 + 0.2389065 * CRL (R² = 0.5355, P = 0.000); HC = 7.710583 + 1.387393 * CRL- 0.0037807 * CRL² (R² = 0.5735, P = 0.000), presented with the fifth, 50th, and 95th percentiles in Figure 1, respectively. The 3rd, 5th, 10th, 25th, median, 75th, 90th, 95th, and 97th percentiles of the BPD and HC at different gestational ages are shown in Tables 1 and 2, respectively. Reference ranges were constructed.
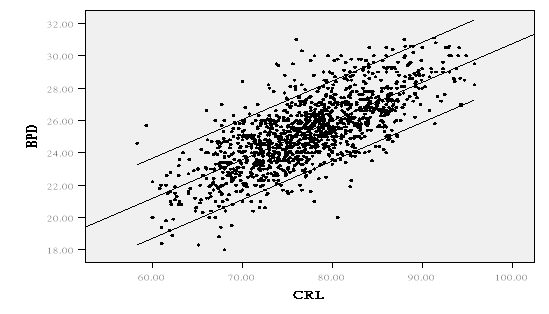
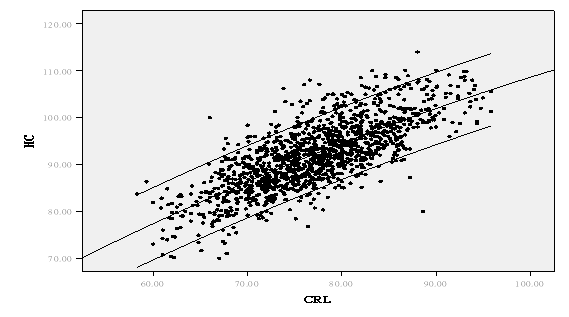
Figure 1:Mean and 95% reference interval for polynomial model fitted to Biparietal Diameter (BPD) (a) and Head Circumference (HC) (b) in relation to crown-rump length (CRL).
Table 1:length of BDP (mm) at 12 - 14 weeks gestation.
| Gestational age (week) | No. of Cases | Mean ± SD | P3 | P5 | P10 | P25 | Median | P75 | P90 | P95 | P97 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 12 | 195 | 22.1 ± 1.3 | 19.1 | 19.8 | 20.6 | 21.4 | 22.3 | 23.0 | 23.7 | 24.0 | 09.2 |
| 13 | 841 | 25.0 ± 1.3 | 22.6 | 22.9 | 23.4 | 24.0 | 25.0 | 25.9 | 26.5 | 27.0 | 22.6 |
| 14 | 315 | 28.0 ± 1.3 | 25.7 | 26.0 | 26.5 | 27.1 | 28.0 | 29.0 | 29.8 | 30.3 | 25.7 |
Table 2:length of HC (mm) at 12 - 14 weeks gestation.
| Gestational age (week) | No. of Cases | Mean ± SD | P3 | P5 | P10 | P25 | Median | P75 | P90 | P95 | P97 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 12 | 195 | 81.5 ± 3.7 | 72.8 | 74.1 | 76.5 | 79.4 | 82.3 | 84 | 84.9 | 86.8 | 87.8 |
| 13 | 841 | 91.0 ± 3.8 | 84.9 | 85 | 85.9 | 88 | 91.3 | 93.8 | 95.7 | 96.6 | 97.6 |
| 14 | 315 | 101.2 ± 3.9 | 95.9 | 96.8 | 97.1 | 98.3 | 100.6 | 104 | 106.7 | 108.26 | 108.8 |
The first observer examined 625 (42%) cases. Mean differences between the two measurements for BPD were −0.4191 (95% CI −1.6869 to 0.8488) and the limits of agreement were −2.3 to 1.5. Mean differences for HC were -0.5429 (95% CI -4.3395 to 3.2538) and the limits of agreement were −2.6 to 1.5. The second observer examined 864 (58%) cases. Mean differences between two measurements for BPD were 0.20 (95% CI −1.0374 to 1.4469) and the limits of agreement were −0.90 to 1.31. Mean differences for HC were −0.1048 (95% CI −3.9036 to 3.6941) and the limits of agreement were −2.1 to 1.9 (Figures 2 and 3).
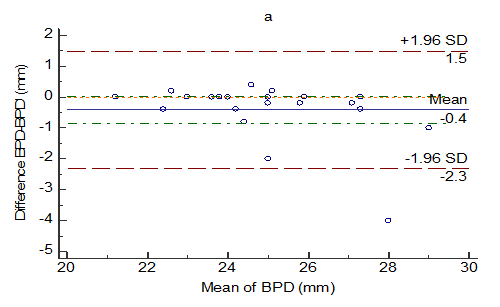
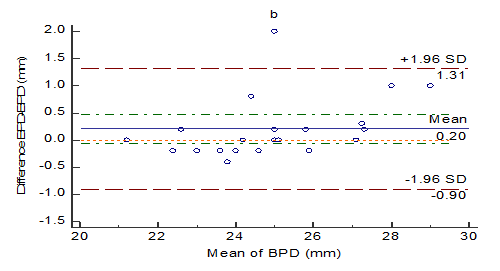
Figure 2:Bland-Altman graphs for intra observer reproducibility of BPD measurements by Observer 1(a) and 2(b).
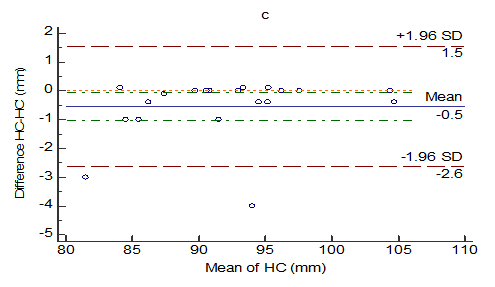
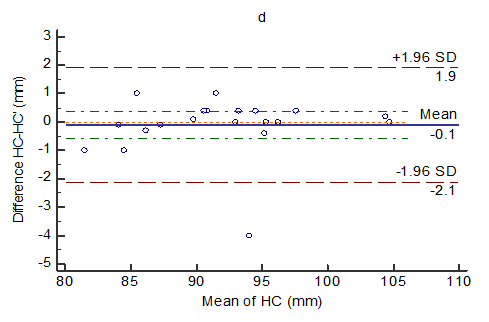
Figure 3:Bland-Altman graphs for intra observer reproducibility of HC measurements by Observer 1(c) and 2(d).
Two independent sample t-tests were used to compare the mean of BPD and HC in our study with the corresponding values in other study on Caucasians[7]. It was demonstrated that the means of BPD and HC in our study were significantly different from that used in Europe (P < 0.001) (Table 3).
Table 3:Comparison of BPD (mm) and HC (mm) betwen two studies (Mean SD) (based on the published data).
| Number | Gestational age | CRL | BPD | HC | |
|---|---|---|---|---|---|
| Present study | 1351 | 13.5 0.55 | 77.1 6.75 | 25.3 2.20 | 92.0 7.16 |
| Salomon’s study | 880 | 12.5 0.57 | 64.3 8.26 | 21.9 2.61 | 79.7 9.3 |
| P-value | 0 | 0 | 0.007 |
Using the equations in the published reference[7], we calculated the mean for each biometric parameter, and they were expressed as Z-scores, based on our new equations. The differences in the mean of BPD and HC among the references are shown in Figures 4.
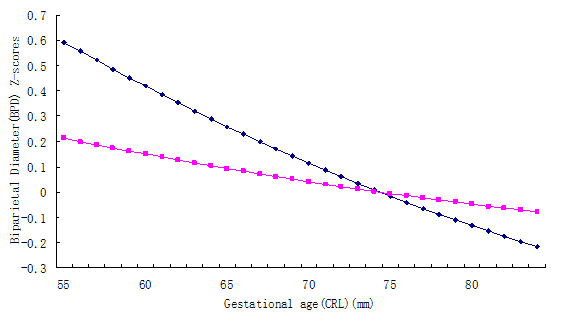
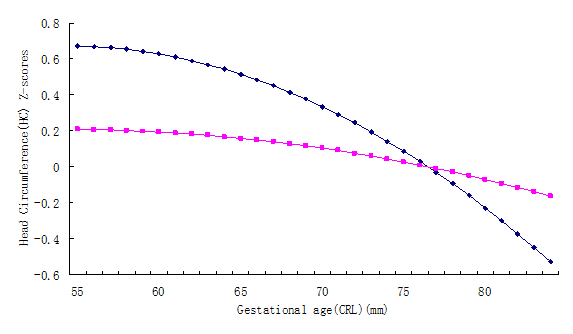
Figure 4:Comparison of our new equations with references A[7] for (a) biparietal diameter and (b) head circumference.
Discussion
Our study established a reference range for BPD and HC at 12 – 14 weeks of gestation in the Chinese population. Previous reports have shown that BPD and HC determined by ultrasound examination correlated with gestation[8,13]. In our study, a slope similar to that of the Caucasians was demonstrated for first trimester head biometry in the Chinese population.
The currently published reference ranges for BPD and HC were mainly from European and American studies[8,13,14]. Some researchers demonstrated that there were no significant differences among the measurements made with static equipment, transabdominal real-time machine, and transvaginal real- time machine. Data from various centers corresponded closely with those of the early investigators[14]. However, variation in fetal head biometry among fetuses of different ethnic origins in the second trimester has been reported[15-18]. It is still controversial whether there is a significant difference in fetal head biometry among fetuses of different ethnic origins in the first trimester.
Z-scores have been increasingly used for comparing individual anthropometric measurements with the reference population[19]. In our study, the differences in the biometry measurement among the references were shown using this method. It was demonstrated that the fetal head biometry in the local Chinese appeared to be different from that of Europeans and Americans in the first trimester of pregnancy[8,13]. The ethnic variation in the biometry measurement cannot be overlooked. On the other hand, growing evidence suggests that although parental maternal height and weight, parity, fetal gender and presentation might have impact on fetal biometry measurement, all these factors may not show remarkable effect until the second and third trimester of pregnancy[20,21].
Fetal biometry measurements are potential candidates in screening for Spina bifida. It is shown that BPD was smaller in spinal bifida at 11 - 14 weeks of gestation. Simple and reproducible BPD at 11 - 14 weeks could detect half of open fetal spina bifida by identifying 5% of pregnancies in first and second- trimester examinations of the fetal spine and cranium by experts[22,23]. Relating the BPD measurement to the Transverse Abdominal Diameter (TAD) could further increase the detection rate of spina bifida[24]. Recent study also suggested that ultrasound standards for head measurements were appropriate for use in the Zika epidemic[25]. Fetal head biometry might have a role in quality control of first-trimester ultrasound examination and may help in the early diagnosis of spina bifida and conditions involving growth abnormalities.
It has been reported that assessment of fetal biometry is largely dependent on the choice of reference charts[26]. Therefore, separate reference charts for the Chinese population should be used in the clinical setting.
References
- 1. Chitty, L.S., Altman, D.G., Henderson, A., et al. Charts of fetal size: 2. Head measurements. (1994) Br J Obstet Gynaecol 101(1): 35-43.
Pubmed || Crossref || Others - 2. Chitty, L.S., Altman, D.G., Henderson, A., et al. Charts of fetal size: 3. Abdominal measurements. (1994) Br J Obstet Gynaecol 101(2):125-131.
Pubmed || Crossref || Others - 3. Chitty, L.S., Altman, D.G., Henderson, A., et al. Charts of fetal size: 4. Femur length. (1994) Br J Obstet Gynaecol 101(2):132-135.
Pubmed || Crossref || Others - 4. Lessoway, V.A., Schulzer, M., Wittmann, B.K., et al. Ultrasound fetal biometry charts for a North American Caucasian population. (1998) J Clin Ultrasound 26(9): 433-453.
Pubmed || Crossref - 5. Leung, T.N., Pang, M.W., Daljit, S.S., et al. Fetal biometry in ethnic Chinese: biparietal diameter, head circumference, abdominal circumference and femur length. (2008) Ultrasound Obstet Gynecol 31(3): 321-327.
Pubmed || Crossref || Others - 6. Salomon, L.J., Alfirevic, Z., Berghella, V., et al. Practice guidelines for performance of the routine mid-trimester fetal ultrasound scan. (2011) Ultrasound Obstet Gynecol 37(1):116-126.
Pubmed || Crossref || Others - 7. Salomon, L.J., Alfirevic, Z., Bilardo, C.M., et al. ISUOG practice guidelines: performance of first-trimester fetal ultrasound scan. (2013) Ultrasound Obstet Gynecol 41(1):102-113.
Pubmed || Crossref - 8. Salomon, L.J., Bernard, J.P., Duyme, M., et al. Revisiting first-trimester fetal biometry. (2003) Ultrasound Obstet Gynecol 22(1):63-66.
Pubmed || Crossref || Others - 9. Hadlock, F.P., Shah, Y.P., Kanon, D.J., et al. Fetal crown-rump length: reevaluation of relation to menstrual age (5-18 weeks) with high-resolution real-time US. (1992) Radiology 182(2): 501-505.
Pubmed || Crossref || Others - 10. Bland, J.M., Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. (1986) Lancet 1(8476): 307-310.
Pubmed || Crossref || Others - 11. Bland, J.M., Altman, D.G. Applying the right statistics: analyses of measurement studies. (2003) Ultrasound Obstet Gynecol 22(1): 85-93.
Pubmed || Crossref || Others - 12. Royston, P., Wright, E.M. How to construct 'normal ranges' for fetal variables. (1998) Ultrasound Obstet Gynecol 11(1): 30-38.
Pubmed || Crossref || Others - 13. Jeanty, P., Cousaert, E., Hobbins, J.C., et al. A longitudinal study of fetal head biometry. (1984) Am J Perinatol 1(2):118-128.
Pubmed || Crossref - 14. Hadlock, F.P. Sonographic estimation of fetal age and weight. (1990) Radiol Clin North Am 28(1): 39-50.
Pubmed - 15. Salomon, L.J., Duyme, M., Crequat, J., et al. French fetal biometry: reference equations and comparison with other charts. (2006) Ultrasound Obstet Gynecol 28(2): 193-198.
Crossref || Others - 16. Sotiriadis, A., Eleftheriades, M., Chatzinikolaou, F., et al. National curves of foetal growth in singleton foetuses of Greek origin. (2016) Eur J Clin Invest 46(5): 425-433.
Pubmed || Crossref - 17. Kwon, J.Y., Park, I.Y., Wie, J.H., et al. Fetal biometry in the Korean population: reference charts and comparison with charts from other populations. (2014) Prenat Diagn 34(10): 927-934.
Pubmed || Crossref || Others - 18. Araujo Junior, E., Martins Santana, E.F., Martins, W.P., et al. Reference charts of fetal biometric parameters in 31,476 Brazilian singleton pregnancies. (2014) J Ultrasound Med 33(7): 1185-1191.
Pubmed || Crossref || Others - 19. Salomon, L.J., Bernard, J.P., Duyme, M., et al. Feasibility and reproducibility of an image-scoring method for quality control of fetal biometry in the second trimester. (2006) Ultrasound Obstet Gynecol 27(1): 34-40.
Pubmed || Crossref - 20. Rizzo, G., Prefumo, F., Ferrazzi, E., et al. The effect of fetal sex on customized fetal growth charts. (2016) J Matern Fetal Neonatal Med 29(23): 3768-3775.
Pubmed || Crossref || Others - 21. Ghi, T., Cariello, L., Rizzo, L., et al. Customized Fetal Growth Charts for Parents' Characteristics, Race, and Parity by Quantile Regression Analysis: A Cross-sectional Multicenter Italian Study. (2016) J Ultrasound Med 35(1): 83-92.
Pubmed || Crossref || Others - 22. Bernard, J.P., Cuckle, H.S., Bernard, M.A., et al. Combined screening for open spina bifida at 11-13 weeks using fetal biparietal diameter and maternal serum markers. (2013) Am J Obstet Gynecol 209(3): 223 e1-5.
Pubmed || Crossref || Others - 23. Bernard, J.P., Cuckle, H.S., Stirnemann, J.J., et al. Screening for fetal spina bifida by ultrasound examination in the first trimester of pregnancy using fetal biparietal diameter. (2012) Am J Obstet Gynecol 207(4): 306 e1-5.
Pubmed || Crossref || Others - 24. Simon, E.G., Arthuis, C.J., Haddad, G., et al. Biparietal/transverse abdominal diameter ratio ≤ 1: potential marker for open spina bifida at 11-13-week scan. (2015) Ultrasound Obstet Gynecol 45(3): 267-272.
Pubmed || Crossref || Others - 25. Marrs, C.C. The ultrasound standards for head measurements are appropriate for use in the Zika epidemic : FOR: Standards are the best tools that are currently available. (2016) BJOG 123(8): 1270.
Pubmed || Crossref - 26. Salomon, L.J., Bernard, J.P., Ville, Y. Analysis of Z-score distribution for the quality control of fetal ultrasound measurements at 20-24 weeks. Ultrasound Obstet Gynecol (2005) 26(7):750-754.
Pubmed || Crossref










