
Growth and Growth Studies in Orthodontics - A Review
Himanshu Trivedi1, Ragni Tandon1, Kamlesh Singh1, Pratik Chandra1, Rohit Kulshrestha2*, Ankit Gupta1, Major Ifran Ahmad3
Affiliation
- 11Department of Orthodontics and DentofacialOrthopedics, Saraswati Dental College, Lucknow, Uttar Pradesh, India
- 2Consulting Orthodontist, Private Practice, Mumbai, India
- 3Army Dental Corps, Punjab, India
Corresponding Author
Rohit Kulshrestha, Consulting Orthodontist, Private Practice, Mumbai, India, E-mail: kulrohit@gmail.com
Citation
Kulshrestha, R., et al. Growth and Growth Studies in Orthodontics - A Review. (2016) J Dent Oral Care 2(4): 1- 5.
Copy rights
© 2016 Kulshrestha, R. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Dentofacial growth; Growth studies; Orthodontics
Abstract
The organization and complexity of growth and development is clearly evident in the changes that take place in the head and face.Craniofacial growth is a complex process. A thorough understanding of the principles or concepts of growth will enable to meticulously plan the treatment, and also understand the normal variations from abnormalities.The basic control of growth, both in magnitude and timing, is located in the genes. The main potential for growth lies in the genes. Many growth studies have been done over the years and the information received from them has been priceless. Extensive research work in growth required large scale growth studies. The purpose of this article is to review the various growth studies and their findings in orthodontic literature.
Introduction
Malocclusion and dentofacial deformities arise through variations in developmental patterns and hence must be evaluated against normal development. Orthodontic treatment also involves manipulation of skeletal growth along with dental correction. Clinical orthodontics requires an understanding of dental development and also concepts about physical growth[1]. Human growth involves physical, mental, psychological, social & moral development. The growth of children is studied for two basic reasons:
(1) To assess the health and nutrition of children.
(2) To compare the growth of an individual child with the growth of a large sample ofother children in the same population.
Growth (magnitude and timing) is basically controlled and located in the genes. Twin studies have mentioned that body size, shape, fat deposition and different growth patterns are under genetic control rather than environmental control. Heredity controls both the end result and rate of progression towards the end result. Genetic factors play a leading role in male-female growth differences[2].
Studying the normal changes in the facial complex helps the clinician to identify and diagnose any abnormalities and treat the same. This knowledge enables the clinician to modify the growth which is required to those patients who seek treatment for skeletal malocclusions[3]. An intensive study of the growth of the craniofacial structures will reveal that it involves very complicated anatomically complex processes. There is large inter relationship between the structures and the effects and causes of these relationships are evident[4]. Correlated growth studies have made their imprints upon researchers all over the world. The studies of growth and development are used to an advantage by researchers. These growth studies have taken longitudinal data of over 10,000 children in different parts of the world. The data derived from these studies has been summarised and many standard norms have been made from this. The pioneers in the commencement of these large scale growth studies are - Todd, Broadbent, Humphries, Waldo, Lewis etc. The data obtained from these studies has helped tremendously in the development of orthodontics as a whole. The purpose of this article is to highlight the iconic growth studies which had been conducted in the past and to show the methodology by which they were undertaken. The historic growth studies which have been completed are.
Bolton-brush growth study
The Bolton-Brush Growth Study consisted of the world’s most extensive data source of longitudinal human growth. The Brush Study was started in 1926 by Prof. T Wingate Todd and his fellow research associates. They examined normal human mental, growth and development. The Bolton Study concentrated only on growth and development of the craniofacial structures and dentition. It was started in 1929 by Holly Broadbent, Sr. the radiographs wereused to study the physical growth changes which take place in the bones of the body with time. The radiographs were taken of the same individuals on a yearly basis for the sole purpose of determining how the body grows (Figure 1).

Figure 1: Bolton-Brush Growth Study.
There were over 6,000 research subjects with over 2,800 of those subjects participating in both the studies. In 1970 Holly Broadbent Jr, the Brush Inquiry and Bolton Study collections combined together and formed the Bolton-Brush Growth Study Centre, which is currently located at the Case Western Reserve University School of Dental Medicine. The Bolton-Brush Centre has records of more than 200,000 radiographs of the head (lateral and frontal views) and various joints of the body (elbow, shoulder, wrist/hand, pelvis, knee, and ankle/foot). Radiographic data and handwritten notes were taken regarding nutritional, dental, medical health and disease history of all the patients. Psychological and mental tests were also conducted annually as part of the Brush Study. Active data which was gathered from the Brush Inquiry stopped in 1942 while the Bolton Study continued gathering data until 1959.
More than 4,000 children from Cleveland had full body x-rays and were included in the Bolton-Brush Growth Studies on normal, healthy development. The youngest child was 3 months old at the start of the study. Elder children were also selected. Their x-rays were taken every three months during the first two years of life and gradually the frequency was reduced after that. The Bolton-Brush Growth Studies have become one of the worlds oldest and longest running studies on normal development and to be a healthy child and now adult[5].
The Burlington growth study
The Burlington Growth Study was the creation of Dr. Frank Popovich, Professor, past Director of Burlington Growth Centre from 1961 to 1989 (Figure 2).
Figure 2: Dr. Frank Popovich.
Once the collection was completed of the longitudinal growth data, he soon realized that he had accumulated one of the largest significant databases for craniofacial growth in the world. The Burlington Growth Centre at the University of Toronto was started by Dr. Robert Moyers in 1952. The specified ages selected for the study were 3, 6, 8, 10, and 12. Records were obtained yearly on the 3 years old children; at ages 9, 12, 14, 16, 20. On the original 6 year old children records were obtained at 12 and 20 years on the original 12-year-old children. Original sample size of 1258 children was present which represented approximately 90% of the Burlington children in these age groups. Records of 111 siblings of the original study group at various ages and 312 parents were also present. Complete orthodontic records were taken for all children which consisted of 6 Cephalometric radiographs 1 PA cephalogram, 2 oblique (45 deg.), 1 lateral cephalogram in occlusion, 1 lateral with open bite, 1 lateral in rest position (enlargement 9.84%) and 1 hand-wrist radiograph. Dental models, height, weight; history, habits, diseases, ethnic background were also recorded carefully. Details of any orthodontic treatment given at the Bolton Growth Centre alongwith photographs were also taken.
Recently the sample size was extended to 40 years from the original 3 year old sample and to 70 years for the original parent sample. Approximately 8,000 sets of records and 46,746 cephalometric X-rays were present. These samples are one of the world’s largest and important collections of longitudinal craniofacial growth and development data. It was started to help and develop parameters to study the successes of orthodontic treatment. It soon became clear that this massive amount of information would help not only the orthodontic researchers but also other fields like medicine, genetics and anthropology. The anthropometric data has contributed to the understanding of craniofacial growth and development. The largest contribution made by Dr. Popovichwas the development of the Burlington Craniofacial Growth Templates. These templates show the amount and direction of craniofacial growth that occurs in both males and females from the age of 4 to 20 years. These templates are used extensively as a diagnostic tool in orthodontics and as well as incephalometric analysis.
Transverse, anterio-posterior and vertical measurements from these templates provide critical information related to the skeletal structures and spatial orientation of the maxilla, mandible and cranial base. All of these factors are an important part of orthodontic diagnosis. The most important observation relates to the dynamics of facial growth and how the treatment will change and modify the growing face. Faces grow either horizontally, vertically or balanced manner. There are horizontal, vertical and balanced growth patterns which help in distinguishing each individual patient. The growth pattern also helps in making the decision for diagnosis and treatment planning. This data is a very important for future studies of secular change in craniofacial growth and development in Caucasian populations[6].
The Michigan growth study
A longitudinal study was done by Riolo on a sample from the Michigan growth centre. The earliest records were gathered by Byron O Hughes who was then succeeded by Robert Moyers. Sample size consisted of 99 males & 92 female subjects between 4 - 19 years of age. Sample was of European Caucasian origin. The records consisted of series of x-rays, study casts, height, weight and medical records (Figure 3).
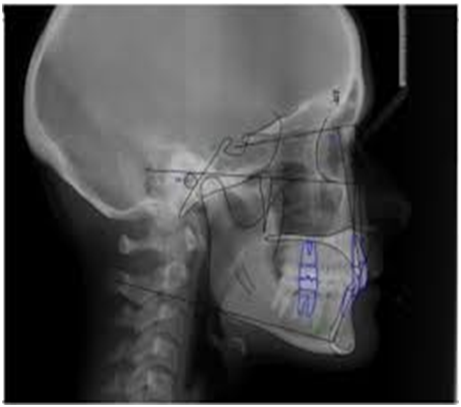
Figure 3: X-rays image with tracing.
Study done by Barry Grayson et al used existing data from cephalostats and derived analysis in 3-D form which were takenfrom the Michigan growth study data base[7,8].
The Denver child growth study
100 children of each sex at each age were taken for this study. The records taken were varied from 2 to 20 years. The subjects were of Caucasian origin. The records taken were lateral and PA view cephalograms and plaster casts. No summary of record sets exists and records do not appear available for general use. Nanda et al evaluated age changes in the morphology and position of the nose, based on a sample from this study[9].
The Iowa child welfare study
The study was done under Samir Bishara. It is a longitudinal study which began with 20 males and 15 female aged 4 yearsand they were followed till 17 years of age. The samples used in this study were non-orthodontically treated patients of entirely Caucasian origin. The records were lateral and PA views radiographs and dental casts. The changes in facial dimensions & relationships as well as in height were evaluated on the basis of this study[10].
The Forsyth twin study
The study was done under the direction of C.F.A Moorrees. The aim of this study was to observe the dental and facial development of 414 twins. The sample size consisted of records for 3 samples of twins for whom complete records are available from 6 - 10 years, 10 - 16 years, and 6 - 16 years. The records were the series of x-rays, casts, height and weight records[11].
The Meharry growth study
The aim of this study was to evaluate the craniofacial growth in the Afro-American children using serial cephalometric radiographs. A longitudinal record of 160 American black subjects wasfollowed from 6 - 14 years. The records were series of x-ray films, casts, photos, medical records taken every 6 months till age14 and annually thereafter[12].
The KrogmanPhiladelphia growth study
The records were originally gathered by Wilton MKrogman and then on by Sol Katz and has been a subject for a number of publications on physical anthropology (Figure 4).
Figure 4: Wilton MKrogman
The sample size consisted of mixed sample of 600 white children, a sample of 150 black children followed from 12 - 18 years, 410 sets of twins; orthodontically treated patients and some records of cleft palate subjects. The records were the series of lateral, PA view and hand wrist x-rays[13].
The Fels growth study
Lewis et al evaluated pubertal growth spurts in cranial base and mandible and studied its variation in individuals based on a sample from the Fels study. The samples were almost exclusively Caucasian with approximately 2% black subjects. The sample size was more than 400 subjects and few of them had history of orthodontic treatment. The subjects were first recorded at 3 months with follow up records every 6 months for 5 years. After 6 years the records were obtained on an annual basis. The Records were the lateral jaw films, hand wrist x-rays[14].
Implant Studies (Arne Bjork)
Prediction of mandibular growth rotation[15]
The technique in which metal implants are inserted in bone has been used in animals for more than a century, but the application of the method in craniometric studies of growth in man has been recently discussed. Bjork’s investigation, which was begun in 1951, comprises a mixed longitudinal study of about 100 children aged from 4 to 24 years. By the implant method, it is possible to locate growth and resorption sites in the individual jaws and also to examine individual variations in growth direction and intensity. The marker technique has also proved useful in the analysis of the mechanisms underlying changes in the inter maxillary relationship during growth. This analysis has led to a radical change in previous views and ideas. This applies to the vertical jaw relation, since the implant technique detects considerably greater rotation of the mandible during growth than which may be seen with conventional methods. Since the information gained by the implant technique should be regarded as supplementary to that obtained from conventional x-ray examinations, the results obtained by the two methods can be compared[15].
Growth Studies in Experimental Animals
Histological response to orthodontic and orthopaedic force
During the first half of the twentieth century animal research established the basis for orthodontic tooth movement dogs were used as experimental animal to determine the tissue response to the application of force to individual teeth the role of osteoclasts & osteoblasts in the remodelling of alveolar bone was described and optimum force levels. The experiments in monkeys and rodents used fulltime appliances with occlusal inclined planes to demonstrate the biological response to functional mandibular protrusion. Animal experiments to investigate the biological response to orthodontic and orthopaedic techniques provide a basis for comparison with clinical experience, when we apply similar techniques in the treatment of patients.
Experiments have shown that condylar cartilage is highly responsive to mechanical stimuli (Stockli & Willert, 1971) and to hormonal and chemical agents (Petrovic; Stutzmann). Hinton (1981) reviews temporomandibular joint function to clarify past misconceptions. Clinical experiments and biochemical data shows that temporomandibular joint is an articulation to which forces are transmitted during normal dental function and one that undergoes adaptive remodelling in response to these forces. Harvold (1983) commented on research started in the University of California in 1965 to examine the changes that occur in the internal structure of the bone in response to functional stimulus[16].
Functional regulation of condylar cartilage growth rate
The theory of functional regulation of condylar cartilage growth rate is supported by recent evidence from animal experiments. Fixed occlusal incline planes have been used to change the distribution of occlusal forces in animal experiments investigating the effects of the functional mandibular displacement on mandibular growth and on adaptive changes in the temporo- mandibular joint (Stutzmann & Petrovic, 1979; Mc-Namara 1980). A fundamental study of the relationship between form and function was carried out in animal experiments at the University of Michigan, and the results were summarized by Mc-Namara (1980). The studies evaluated changes in muscle function and related changes in bone growth in the rhesus monkey by a comparison of experimental and control animals as monitored by electromyographic (EMG), cephalometric and histological studies. McNamara concluded that these studies demonstrated the close relationship between functional and structural components of the craniofacial region. The findings were based on the use of fixed occlusal inclined planes that were designed to cause a forward postural displacement of the mandible in all active and passive muscle activity. The pattern of muscle behaviour during the experimental period showed a cyclic change in response to functional mandibular propulsion.
Initial placement of the appliance produced an increase in the overall activity of the muscle of mastication as the animal sought to find a new occlusal position. A distinct change in muscle activity occurred within 1 - 7 days. This was characterized by a decrease in the activity of the masseter muscle and most significantly an increase in function of the superior head of the lateral pterygoid muscle. After 3 weeks a new plateau of muscle activity was reached at a higher level of activity that the pre-treatment record this level of activity persisted for 4 weeks before a further decline in muscle activity over a period of 4 weeks to the level of recorded before treatment. The cycle of changes was complete in 3 months (Figure 5).
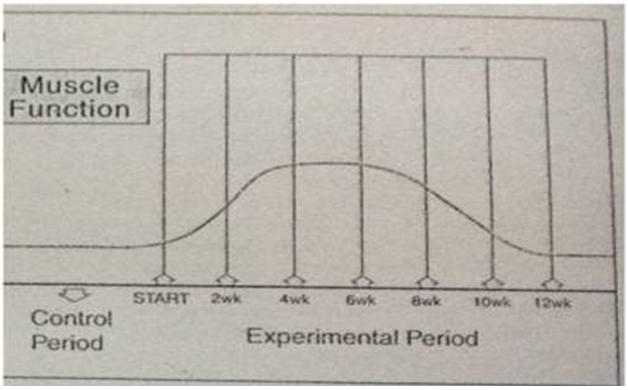
Figure 5: Electromyographyshowing the cycle of change in musclebehaviour.
A similar experimental study at University of Toronto on the effect of placement of a functional appliance on muscle activity showed different conclusions (Sessile et al, 1990). This study used chronically implanted EMG electrodes to identify a statistically significant decrease in postural EMG activity of the superior and inferior heads of the lateral pterygoid and the superficial masseter muscles, which persisted for 6 weeks and returned to pre-treatment levels during a subsequent 6 weeks period. Progressive mandibular advancement of 1.5 - 2 mm every 10 - 15 days did not prevent the decrease in postural EMG activity. The clinical implication of these differing results is that the question of activation of a functional appliance by a single large mandibular displacement or a progressive series of smaller activation is still to be resolved. It is not established whether active muscle contraction or passive muscle tension is the primary stimulus to growth in functional therapy[16].
Conclusion
Growth and development from a new born to adult hood is characterized by a multiplicity of morphological, physiological and psychological changes. Many characteristics of general body growth are also present in the growth of the craniofacial region. The answer to our clinical problems lies not in the development of better appliances but, in a complete understanding of craniofacial growth and its implication in the clinical situation for the appraisal of our treatment modalities that suit the patient better so as to achieve the best results in form of function, esthetics and structural balance. The orthodontist is virtually concerned with facial balance and harmony, because the smile and profile that he is able to mold into a patient’s face is carried forth to meet the real world, it is reasonable for us to speculate about how the success or failure of such treatment can affect the child’s social and psychological well-being. For any clinician to achieve the optimum facial features possible, he must link beyond external manifestations to the underlying changes in the bony foundation that brings them about. The student of facial growth studies must be interested in where growth occurs and what tissues and cells are contributing. He must attempt to differentiate between normal and abnormal growth, and he must, if he is a therapist, understand what patterns can be altered and what techniques to do so are presently available. Many growth studies which have been done, have given us a new perspective about craniofacial growth. It has helped us to evaluate growth and development of different individuals of different age groups. Some growth studies have given us a foundation onwhich to build on and assess growth in different stages of individuals e.g. Bolton brush study, Burlington growth study, Bjork implant studies. In all the study of growth and development is very important for the orthodontist as it helps him to diagnose and assess the case and plan the best treatment plan possible for the patient.
References
- 1. Proffit, W.R., Fields, H.W., Sarver, D.M. Contemporary orthodontics. (2007) Elsevier 4th ed. C.V. Mosby, St Louis:234–267.
- 2. Bishara, S.E. Textbook of Orthodontics. (2001) Saunders Philadelphia PA.
- 3. Sridhar, P.K. Textbook of Craniofacial Growth. (2011) Basic Principles and Practice. 4th Edition: 46-56.
- 4. Schudy, F.F. The Rotation of the Mandible Resulting from Growth: its Implications in OrthodonticTreatment. (1965) the Angle Orthodontist 35(1): 36-50.
- 5. Graber, T.M., Rakosi, T., Petrovic, A.G. Dentofacial orthopedics with functional appliances.(1997) 2nd Edition,St. Louis, Mosby.
- 6. Enlow, D.H., Hunter, W.S. Growth of the face in relation to the cranial base. (1968) Rep CongrEurOrthodSoc44: 321-335.
- 7. Mc.Namara, J.A. (ed.)Craniofacial Growth Series 35, The University of Michigan, Ann Arbor, 1999.
- 8. Subtelny, J.D.A longitudinal study of soft tissue facial structures and their profile characteristics, defined in relation to underling skeletal structures. (1959) Am J Orthod 45(7):481 -507.
- 9. Nanda, R.S. Growth changes in the nasal profile from 7-8 yrs. (1988) AJO 94(4): 317-326.
- 10. Bishara, S., Peterson, J.R. changes in the facial dimensions & relationships between the ages 5-25yrs. (1984) AJO85(3): 238-252.
- 11. Lewis, A. B., Roche, A.F.Pubertal spurts in cranial base & mandible. (1985) AJO 55(1): 17-30.
- 12. Atlas of craniofacial growth in Americans of African descent CFGS.26
- 13. Scott, J.H. The growth of human face. (1954) Proc R Soc Med 47(2):91-100.
- 14. Chaconas, S. Prediction of normal soft tissue facial changes. (1975) Angle Orthod 45(1): 12-25.
- 15. Bjork, A. Prediction Of mandibular growth rotation. (1969) Am J Orthodontics 55(6):585-599.
- 16. William, J,Clark. Twin blocksfunctional therapy, applications of dentofacial orthopedics. (2015)Mosby Elsevier 147(5): 636.










