
Impact of the City Environment on Human Health: The Case of Pollen Allergy in Region of Beni Mellal in Morocco
Sanaa Sabour Alaoui1,2*, Nadia Barje2
Affiliation
- 1Polyvalent Research and Development Laboratory (LPRD)
- 2Polydisciplinary faculty of Beni Mellal, University of Sultan Moulay Sliman
Corresponding Author
Sabour Alaoui Sanaa, Polyvalent Research and Development Laboratory (LPRD), Polydisciplinary faculty of Beni Mellal, University of Sultan Moulay Sliman, Mghila B.P. 592, Beni Mellal, Tel: +212 523424685/ Fax: +212 523424597, GSM: + 212 (0) 618127040, E-mail: sanaa_ala@yahoo.fr
Citation
Sabour Alaoui, S., et al. Impact of the City Environment on Human Health: The Case of Pollen Allergy in Region of Beni Mellal in Morocco. (2017) J Environ Health Sci 3(2): 1-6.
Copy rights
© 2017 Sabour Alaoui, S. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Pollen allergy; Symptoms; Olive tree; Cross-reactivity; Survey
Abstract
Background: Today, the number of allergy is increasing in industrialized countries. The World Health Organization (WHO) classifies allergic diseases to be the fourth in the world of affections. The frequency of respiratory allergy including asthma and allergic rhinitis due to pollen is increasing in the young and urban dwellers in developed countries. The prevention and management of allergy in universities is an area of active interest because allergies and asthma rates among young people continue to increase. The allergic reactions are less serious whereas they can develop into a serious form of asthma and anaphylaxis that can endanger life and require immediate medical care. A better understanding of the prevalence and characteristics of allergy can help guide to strategy of management against development of allergic rhinitis, asthma and anaphylaxis within and outside academic institutions in order to reduce the risk of morbidity and mortality.
Objective: This study was carried out for a characterization of pollen allergy and its relation with the environment in the university establishment in order to propose strategy of management against this disease.
Methods: The project was to study pollen allergy in FPBM in an effective sample of 529 randomly chosen within a range of about 7,000 students. A survey was made for a descriptive studies.
Results: The percentage of students allergic to pollen surveyed in the FPBM was 39%. This percentage was within the confidence interval of all students in the allergic FPBM [35%; 44%] estimated 5% error risk. This results prove that our sample was representative. We also found that the most common symptoms of pollen allergy among its students are the nasal symptoms (sneezing and nasal itching). These symptoms characterize allergic rhinitis. Our study shows that the olive tree is the main allergen causing pollen allergy in the region. This study shows that most students have allergies in the spring season, this could be explained by the pollinisation of olive tree in this period. Our study shows that the majority of surveyed students are allergic to one or two types of plants and the cross-reactivity between pollen and food was the most dominant.
Conclusion: The case reported here is particularly intersting because, to the best of our knowledge, high percentage of allergy to the pollen in the region Beni Mellal-Khenifra has not reported before. Olive tree was the main allergen, this can be explained by the richness of the region of Beni-Mellal-Khénifra with this plant. These results are unexpected, normally these youngsters must present a resistance to the pollen present in the region because they are native and have an adaptation to the environment. But we find an almost quarter of the young people surveyed in the area present the allergy. This allows us to ask several questions about the relationship between environment and the development of allergy.
Introduction
The World Health Organization (WHO) classifies allergic diseases fourth in the world of affections and considers that these diseases are a major public health problem in terms of quality of life, loss of work days or teaching of drug and even mortality cost. According to a WHO estimate, it could reach 50% of the world population in less than ten years (Shahali Y., et al, 2013). For over 40 years, the frequency of respiratory allergies including asthma and allergic rhinitis is increasing in the young and urban dwellers in developed countries (Abou Chakra, et al, 2009; 2011).
Today, the number of allergy is increasing in industrialized countries. Allergies due to pollens affect 10 to 15% of the overall population (Ravault C., et al, 200). Pollen allergy, pollinosis, is a disease linked to the presence in the air, the seasons, more or less quantity of pollen grains from a variety of plants (Abou Chakra, et al, 2009). Pollinosis cause reactions at the contact areas such as respiratory and ocular mucosa and occasionally they may be responsible for skin reactions such as eczema or hive. She is responsible for various symptoms include rhinitis, conjunctivitis, dry cough, skin disorders and allergic asthma. Nasal and ocular manifestations are central to the clinical symptoms (Kirmaz C., et al, 2005; Wagner A., et al, 2016).
In allergic cases, the encounter with the allergen in a particular context (sensitization phase) is determinant. This context is defined by the nature of the allergen, quantity, its modes, time and frequency in the body penetration and also by history immune (infection, inflammation...) of the individual (Sahali, Y., et al, 2013).
The allergic reactions are less serious whereas they can develop into a serious form asthma and anaphylaxis that can endanger life and require immediate medical care.
Anphylaxis is a severe potentially fatal, system allergic reaction that occurs suddenly after contact with allergy causing substance (pollen, food, drugs, stinging insects) (Ramón GD., et al, 2017). It is characterized by compromise of airways, breathing circulatory problems and is usually associated with changes in the skin and mucosa (Ramón GD., et al, 2017).
The environment (pollution, lifestyles) and climate change proved to play an important role in the increased prevalence of allergic diseases (D’Amato G., et al, 2016).
The awareness phase is defined as the exposure to the allergen, but it never enters the body as pure protein but often accompanied by other compounds or non-allergenic proteins, molecules or organic or inorganic particles, bacteria, viruses, mushrooms (Sahali, Y., et al, 2013). The adjuvant role of the environment associated with climate change playing on the length of exposure, the dispersion of pollen and on the distribution of species of trees and plants (rise in latitude) is involved in the increase in cases of allergy observed in recent years (Bonofiglio T., et al, 2013; D’Amato G., et al, 2016).
The impact of climate change on the occurrence of allergic diseases can be evaluated on the basis of changes in time of appearance of specific phenological phases, the intensity of pollination, or the number of days when concentrations result in allergic symptoms. One of the most important analysis is the evaluation of how these changes can be reflected in reference to the start of the pollen season for some allergenic plant taxa (Perveen A., et al, 2015).
The health effects of climate change are causing an increase in the prevalence of allergic respiratory diseases, exacerbations of chronic obstructive pulmonary disease, and premature mortality (Katotomichelakis M., et al, 2016). Climate change associated with the greenhouse effect is causing adverse health effects among the most vulnerable populations, such as the elderly, children and those in socioeconomic strata in distress (D’Amato G., et al, 2015; D’Amato G., et al, 2016).
In Morocco, allergic diseases are becoming more frequent (Mallol J., et al, 2013). However, no official data are available on the prevalence of asthma and allergic rhinitis (Kettani SE., et al, 2009). This lack of epidemiological data prompted us to carry out a study to determine the prevalence of allergy amongst young people in the Béni Mellal region.
Materials and Methods
Study area
The region of Beni Mellal-khénifra is one of the twelve Moroccan regions created by the territorial division 2015; it includes the region of Tadla-Azilal and the provinces of khénifra and Khouribga, located in the center of the country. It encompasses the plain of Tadla, between the high atlas and the middle atlas its center is Béni Mellal. The region is characterized by a very continental climate and the precipitation slope varies between 300 and 750 mm depending on the year. Agriculture represents the dominant activity at the level of the region both by the jobs offered and by the effects induced on the regional economy.
We chose the Polydiscipline Faculty of Beni Mellal (PFBM), as a place for the study of pollen allergy; it is a public institution of higher education, which receives each year thousands of young students from different places of this region that is characterized by its rich vegetation.
Study Participants
The project consists to study prevalence of pollen allergy in a sample size of 529 students (female 316, male 213), chosen randomly from a set of about 7000 students from PFBM. A questionnaire (see annex) was prepared for this study.
Questionnaire
We conducted a questionnaire at PFBM on 529 students as a sample. These students were asked to study the prevalence of pollen allergy.
Several categories of questions were used in our questionnaire: personal data (sex, age, habitat), dichotomous question (the existence of pollen allergy), multiple choice questions to know plants that cause pollen allergy, allergic symptoms (ocular, nasal and asthmatic symptoms), onset of symptoms (summer, spring, fall and winter), the study of the existence of another disease, the existence of cross-allergy and the type of treatment used.
Statistical Analysis
Confidence interval: The study of proportion of allergy in the PFBM student is important feature in our study but its exact value cannot be given since it is impossible to have comprehensive information about the population. We estimate its exact value by the confidence interval with an error risk of 5%.
The method: At the risk of error 5%, the unknown proportion of a population, which can be deduced from a random sample, is within the confidence interval of the form:

With:
p = proportion of the sample
α = risk of error equal to 5%
n = sample size
Z_(1-(α)/2) = A normal centered reduced variable for the case of n > 30
Statistical analysis of the data was performed using excel and handled by the software of statistical processing (SPSS), version 22. Variables were considered statistically significant at p values of less than 0.05.
The information about the number of young people affected by pollen allergy in the FPBM was statistically evaluated by measuring the prevalence P.
P = p * 100
Chi-Square Test of Independence
Chi-Square test of independence is used to determine if there is a significant relationship between gender (male vs. female) and allergy. The chi-square statistic was calculated by using the STATISTICA 7 Software.
Results
Pollen allergy in PFBM: The proportion of pollen allergy students in the PFBM was estimated by confidence interval test. From the table of the law N (0, 1): Z_(1-(α/2)) ≅ 2
The proportion of allergic students in the random sample within the poly-disciplinary faculty, number n = 529, is:
| Sex | Female | Man |
|---|---|---|
| Number of allergic students | 128 | 78 |
p = (128 + 78)/529 ≅ 0,39
p = 0,39 * 100 = 39%
That is, in our sample we have almost 39% of the students who are allergic to pollen according to the following table of data:
At the risk of error 5%, the unknown proportion of a population, which can be deduced from a simple random sample, is within the confidence interval of the form:
As a result at the risk of error 5%, the proportion of allergy students in the PFBM is given by confidence interval: [0.35; 0.44]. That is, in all students, between 35% and 44% are allergic to pollen.
According to the analysis of the survey results conducted at the PFBM, the prevalence of allergic students to pollen surveyed is 39% and 61% for students not allergic to pollen (figure1). It means that the pollen allergy is present in almost quarter of the students of PFBM. The 39% allergic students enter in the confidence interval (35%; 44%) calculated for all students of the faculty at the risk of error 5%. These results show that our sampling of 529 students is representative of all students of PFBM.
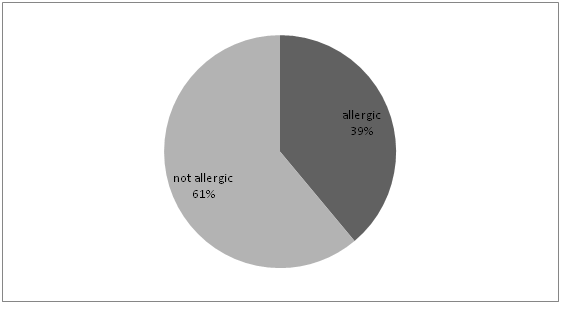
Figure 1: Distribution of students survey allergic and non-allergic to pollen of PFBM.
Pollen allergy and sex: The figure 2 and table 2, show that 40.5% of female students are allergic to pollen compared to all female students while 36.6% of male students are pollen allergy compared to all male students surveyed. We concluded that this difference beteween female and male are not significant.
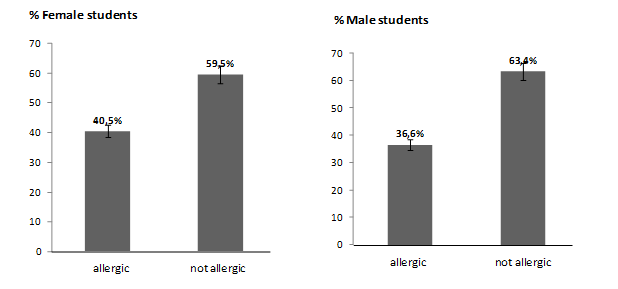
Figure 2: Distribution of allergic and non-allergic surveyed students to pollen of PFBM according to the category of sex.
Table 2: Distribution of allergic and non-allergic students according to the sex of the FPBM.
| Allergy | total | |||
|---|---|---|---|---|
| Number of allergic students | Number of non allergic students | |||
| sex | Female | 128 | 188 | 316 |
| Male | 78 | 135 | 213 | |
| Total | 206 | 323 | 529 | |
From the STATISTICA 7 Software and the table of Chi-Square, we have the following results:
Khi² (the observed value) = 0.81
Khi² (the critic value) = 3.48
DF = (2-1)(2-1)
p-value = 0,3686
Thus, we can conclude that there is independence between the two factories sex and presence of allergy, at the risk level 5%.
Allergens responsible of pollen allergy: The main allergens responsible of pollen allergy in students PFBM are shown in Figure 3. We observed that the plants that promote allergy of pollen in students surveyed are olive (38%), orange (16%), almonds (12%), peach (11%) and pomegranate (10%). It is concluded that the olive tree is the main allergen causing pollen allergy. We can explain these results by the richness of the region of Beni Mellal-Khénifra by these trees and mainly the olive tree.
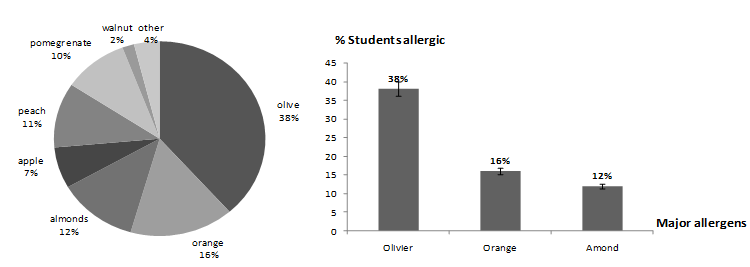
Figure 3: Distribution of allergens responsible for pollen allergy in the allergic students PFBM.
Relationship between seasonal variation and pollen allergy: It is observed in Figure 4 that the percentage of pollen allergy of allergic students depending of the season is as follows: 10% in autumn, 20% in winter, 64% in spring and 5% in the summer. From these results, it is found that the pollen allergy is frequently in the spring compared to other seasons.
Since it was found that the olive tree is the main allergen responsible for the allergy to pollen and also we know that the olive tree pollination season is spring, this explains the increasing number of students allergic to pollen in this season.
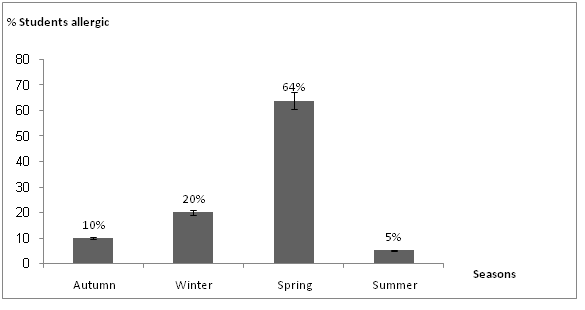
Figure 4: Distribution of pollen allergy in allergic students depending of the seasons.
Relationship between the number of types of plants and pollen allergy: The results show that 52% of young people are allergic to more than one plant while 47% are allergic to a single plant. Analysis of the results (Figure 5) shows that the percentage of allergic students to one plant is 47%, two plants 31%, three plants 17%, four plants 4% and more than four 1%. We find that the majority of surveyed students are allergic to more than on types of plants.
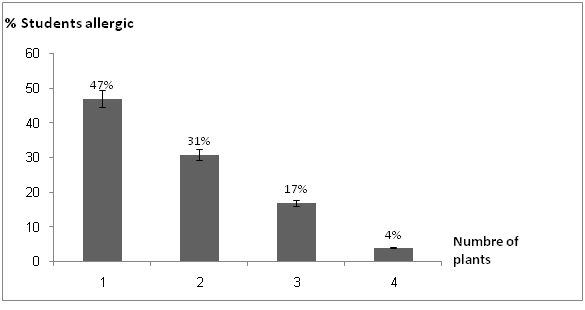
Figure 5: Distribution of students surveyed at PFBM depending on the number of types of plants responsible for pollen allergy.
Symptoms due to pollen allergy among students allergic: The most common symptoms responsible of the allergy to pollen among students in the PFBM are: sneezing (70%) and eyes watering (59%) and nasal itching (51%) (Figure 6). These results show that the nasal symptoms and ocular symptoms are the most dominant.
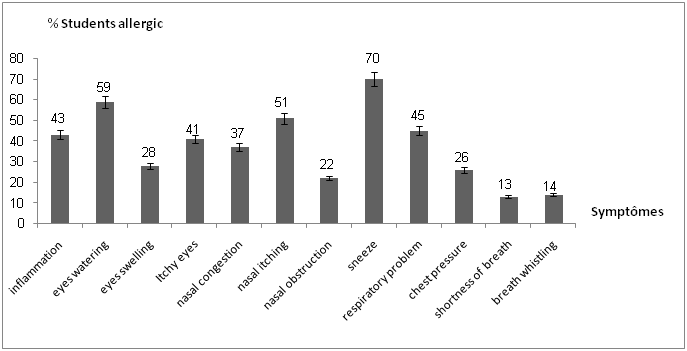
Figure 6: Distribution of symptoms due to pollen allergy among students surveyed the PFBM.
Cross-reactivity between pollen and other allergens: Questionnaire data carried out show that the cross-reactivity in the allergic students in PFBM between pollen allergen and food is the most dominant (27%). While cross-reactivity pollen allergy-dust is 16% and pollen allergy-animals is less common 5% (Figure 7).
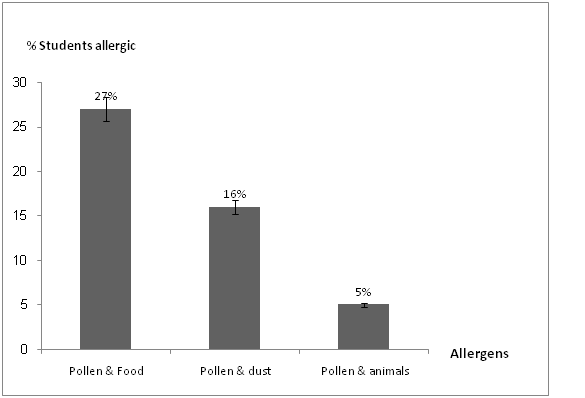
Figure 7: Distribution of cross-reactivity between pollen and other allergens in the surveyed students PFBM.
Discussion
Allergy diseases are currently a global public health problem. The scarcity of epidemiological studies in Morocco prompted us to carry out this study which the objective is to determine the prevalence of pollen allergy in the Beni Mellal region.
The percentage of students allergic to pollen surveyed in PFBM is 39%, this percentage might be explained by the wealth of the region in vegetation. This percentage enter into the confidence interval [35%; 44%] estimated at 5% error risk, of all allergic students in PFBM, which proves that our sample is representative. We show at the first time that almost quarter of students had hypersensitivity to pollens.
All students surveyed are from the region of Beni Mellal. These results are unexpected, normally these youngsters must show resistance to pollen present in the region but we find the opposite. However, constraints such as climate change have known the region over the past few years, notably global warming is favoring the problem of increasing pollination.
We suggest that climate and environmental factors have the ability to influence local botany and aerobiology by increasing number of tree pollen.
We found also that the female and male allergic percentages are not significant. We concluded that there is independence between the two factories sex and presence of allergy.
Our study shows that the olive tree is the main allergen causing pollen allergy because the region Beni Mellal-Khénifra is rich in this plant. Olive pollen is important cause of pollinosis and is considered as one of the most important causes of respiratory allergic disease in mediterranean region.
The results show that 52% of young people are allergic to more than one plant while 47% are allergic to a single plant. These results suggest the possibility that pollen allergy over time weakens the immune system and makes it susceptible to aggression with other pollen or suggests the possibility of aggression with pollen that presents molecular resemblances or proteins that share common epitopes.
The most common symptoms of pollen allergy among of students are nasal (sneezing and nasal itching) and ocular. These manifestations are central to the clinical symptoms of allergic rhinitis.
This study shows that most students 64% have allergies in the spring season; this could be explained by the pollination of olive trees in this period (from April to June). Our study shows also that pollen allergy is present in the other seasons, autumn 10%, winter 20% and summer 5%. These results can be explained by the climate change that influence the duration and intensity of pollen seasons could in hand with the air pollution contributes to the increase in respiratory allergies and asthma (D’Amato G., et al, 2015; D’Amato G., et al, 2016) in this region.
Our study shows also that cross-reactivity between pollen and food is the most dominant and then found pollen allergy cross-dust. Our results confirm other recent research on the evidence of this reactivity between pollen and food and which tries to understand the mechanism (Popescu F-D, 2015). Research shows that pollinosis patients often display adverse reactions upon ingestion of plant-derived foods as a result of IgE cross-reactive epitopes shared by pollen and food allergen sources (Bousquet J., et al, 2008; Popescu F-D, 2015).
Conclusion
Using the questionnaire as a screening tool for diagnosing the presence of pollen allergic in students of PFBM, we confirmed the high rates of pollen allergic students and found that the prevalence of allergy in students varies across seasons. We suggest that the seasonal variation associated with the climate change influences the duration and intensity of pollen seasons in region.
Our results allow us to ask several questions about the causes of allergy and to look for strategies to control the epidemic of this disease in these universities.
Acknowledge:
We thank students of Polydisciplinary Faculty of Beni Mellal for their collaboration and support in the development of this document.
Conflict of interest:
The authors declare that they have no competing interests.
References
- 1. Abou Chakra, O., Rogerieux, F., Poncet, P., et al. Ability of pollen cytoplasmic granules to induce biased allergic responses in a rat model. (2011) Int Arch Allergy Immunol 154(2): 128–136.
Pubmed || Crossref || Others - 2. Abou Chakra, O., Sutra, J-P., Rogerieux, F., et al. Immunological Interactive Effects between Pollen Grains and Their Cytoplasmic Granules on Brown Norway Rats. (2009) World Allergy Organ J 2(9): 201–207.
Pubmed || Crossref || Others - 3. Bonofiglio, T., Orlandi, F., Ruga, L., et al. Climate change impact on the olive pollen season in Mediterranean areas of Italy: air quality in late spring from an allergenic point of view. (2013) Environ Monit Assess 185(1): 877–890.
Pubmed || Crossref || Others - 4. Bousquet, J., Khaltaev, N., Cruz, A.A., et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). (2008) Allergy 63(Suppl 86): 8–160.
Pubmed || Crossref || Others - 5. D’Amato, G., Pawankar, R., Vitale, C., et al. Climate Change and Air Pollution: Effects on Respiratory Allergy. (2016) Allergy Asthma Immunol Res 8(5): 391–395.
Pubmed || Crossref || Others - 6. D’Amato, G., Holgate, S.T., Pawankar, R., et al. Meteorological conditions, climate change, new emerging factors, and asthma and related allergic disorders. A statement of the World Allergy Organization. (2015) World Allergy Organ J 8(1): 25.
Pubmed || Crossref || Others - 7. Katotomichelakis, M., Danielides, G., Iliou, T., et al. Allergic sensitization prevalence in a children and adolescent population of northeastern Greece region. (2016) Int J Pediatr Otorhinolaryngol 89: 33–37.
Pubmed || Crossref || Others - 8. Kettani, S.E., Lotfi, B., Aichane, A. Prevalence of allergic rhinitis in a rural area of Settat, Morocco/Prevalence de la rhinite allergique en milieu rural a Settat (Maroc). (2009) East Mediterr Health J 15(1): 167–178.
Pubmed || Crossref || Others - 9. Kirmaz, C., Yuksel, H., Bayrak, P., et al. Symptoms of the olive pollen allergy: do they really occur only in the pollination season? (2005) J Investig Allergol Clin Immunol 15(2): 140–145.
Pubmed || Crossref || Others - 10. Mallol, J., Crane, J., von Mutius, E., et al. The International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three: a global synthesis. (2013) Allergol Immunopathol (Madr) 41(2): 73–85.
Pubmed || Crossref || Others - 11. Perveen, A., Khan, M., Zeb, S., et al. Impact and correlation of environmental conditions on pollen counts in Karachi, Pakistan. (2015) Iran J Allergy Asthma Immunol 14(1): 83–90.
Pubmed || Crossref || Others - 12. Popescu, F-D. Cross-reactivity between aeroallergens and food allergens. (2015) World J Methodol 5(2): 31–50.
Pubmed || Crossref || Others - 13. Ramón, G.D., Croce, V.H., Chérrez Ojeda, I. Anaphylaxis in a 4-year-old male caused by contact with grasses: a case report. (2017) World Allergy Organ J 10(1): 5.
Pubmed || Crossref || Others - 14. Ravault, C., Kauffmann, F. Validity of the IUATLD (1986) questionnaire in the EGEA study. International Union Against Tuberculosis and Lung Disease. Epidemiological study on the Genetics and Environment of Asthma, bronchial hyperresponsiveness and atopy. (2001) Int J Tuberc Lung Dis 5(2): 191–196.
Pubmed || Crossref || Others - 15. Shahali, Y., Brazdova, A., Calleja, M., et al. Indoor, long-term persistence of cypress pollen allergenic potency: a 10-month study. (2013) Ann Allergy Asthma Immunol 111(5): 428–430.
Pubmed || Crossref || Others - 16. Sahali, Y., Poncet, P., Senechal, H. Cupressaceae pollinosis and air pollution. (2013) Rev Fr Allergol 53(5): 468-472.
Pubmed || Crossref || Others - 17. Wagner, A., Szwed, A., Buczyłko, K., et al. Allergy to apple cultivars among patients with birch pollinosis and oral allergy syndrome. (2016) Ann Allergy Asthma Immunol 117(4): 399–404.
Pubmed || Crossref || Others










