
Intracranial Parasagittal Epidural Abscess: Another Consideration for the Etiology of Acute Headache and Fever Following a Minor Head Injury
Williamson K. L2
Affiliation
- 1Department of Neurological Surgery, Legacy Emanuel Medical Center, 2801 N. Gantenbein Ave, Portland, OR 97227, USA.
- 2Department of Neurological Surgery, University of California Irvine, 200 S. Manchester Ave, Suite 210, Orange, CA 92868, USA.
Corresponding Author
Jeff W. Chen, Neurological Surgeon and Director of NeuroTrauma, Department of Neurological Surgery, University of California, Irvine, USA. Tel: (714) 456-6966, Fax: (714) 456-8202; E-mail: effewc1@uci.edu
Citation
Chen J. W., et al. Intracranial Parasagittal Epidural Abscess: Another Consideration for the Etiology of Acute Headache and Fever Following a Minor Head Injury (2015) Int J Neurol Brain Disord 2(1): 1- 4.
Copy rights
© 2015 Chen J. W. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Intracranial epidural abscess; Head trauma; Traumatic brain injury; Pediatrics; Neurosurgery; Sinusitis; Urinary tract infection; Streptococcus intermedius
Abstract
A previously healthy seven-year-old girl, who suffered a minor head injury, experienced diagnostic complications spanning two weeks, resulting from an intracranial epidural abscess. Originally diagnosed with cephalgia and a urinary tract infection, which were unresponsive to antibiotics, secondary workup revealed a large bifrontal epidural lesion. She was transferred to our neurosurgery services for further management and workup of the lesion. Magnetic resonance imaging demonstrated an enhancing anterior parasagittal fluid collection that was suggestive of an infection. Burr-hole surgery directly over the lesion confirmed the diagnosis of brain abscess. Irrigation and drainage was done, and her recovery was rapid and uncomplicated with the subsequent treatment with appropriate antibiotics. A possible etiology for this unusually located abscess is that the patient had a hemorrhage into this location from the initial injury. This subsequently became infected after a urinary tract infection or sinusitis. This case may be a useful reference for identifying patients with a brain abscess after a minor head injury, this occurring without direct invasion of the region of concern with a known foreign body, the usual mechanism after a traumatic brain injury.
Introduction
Intracranial epidural abscesses (IEA) are an uncommon, but potentially life-threatening condition, requiring accurate diagnosis and therapeutic management. The diagnosis of a brain abscess is often unsuspected because of vague and non-specific symptoms and presentation without overt neurological impairments[1-7]. The etiology of the brain abscess can be contiguous with the source of infection, likely secondary to a primary source (middle ear, mastoid cells, or paranasal sinuses in 25% - 50% of cases), hematogenous dissemination (20% - 35% of cases), or trauma, which can incorporate obvious damage to the brain and surrounding structures, or arise as a complication of a neurosurgical procedure[2,8]. Of note, a brain abscess is cryptogenic in up to 10%-35% of cases, increasing the likelihood of a misdiagnosis[2,4,8]. Diagnostic connections between minor traumatic head injury and IEA are infrequently considered in the differential for patients presenting with headaches, fevers, and no neurological abnormalities. Commonly reported cases show an obvious link between IEA and severe traumatic brain injuries requiring neurosurgical intervention, where the abscess arises from the initial traumatic insult or from the invasive surgery[2,5,6]. We present here a case of a seven-year-old girl who suffered a mild traumatic head injury resulting in a large bifrontal epidural abscess, with markers for systemic infection, but no obvious neurological abnormalities.
History and Examination
A seven-year-old girl was admitted to our hospital following a complicated two-week symptomatic/diagnostic history after suffering a mild head injury, without documented loss of consciousness. The family reports that the patient suffered an unwitnessed fall off a couch striking the back of her head. They noted a small cephalohematoma over the right occipital-temporal region. There was no documented loss of consciousness. 48-hours after the head injury she began experiencing acute headaches and intermittent fever of 38.3-39.4°C, unresponsive to over-the-counter pain medications. One week passed with these unrelenting symptoms, and she was taken to a local emergency department (ED). Work-up was done for infection. Urinary analysis was positive for leukocyte esterase and cultures identified Escherichia coli at 60,000 to 70,000 CFU/mL. She appeared appropriate in all other systems and was discharged with a diagnosis of cephalgia and urinary tract infection (UTI), with counsel to start a regiment of Bactrim antibiotics by mouth for the UTI.
The patient re-presented to the outside ED three days later with worsening symptoms, including photophobia, stiff neck, headache, poor appetite and a reoccurring fever of 38.3 - 39.4°C, (unresponsive to the course of Bactrim). Her disposition and alertness were normal, with no acute neurological distress. She underwent emergent computed tomography (CT) studies, revealing an abnormal epidural iso- to hypo-dense fluid collec-tion (1 cm in thickness) following the sagittal anterior calvarium, with mass effect on the sagittal sinus and bilateral anterior frontal cortex. Blood examination of inflammatory markers showed white blood cell (WBC) counts of 10.8 x 103/μL and erythrocyte sedimentation rate (ESR) of 98 mm/hr (Time = 0 day). At this point, she was transferred to our hospital for further workup of this epidural enhancement Figure 1.
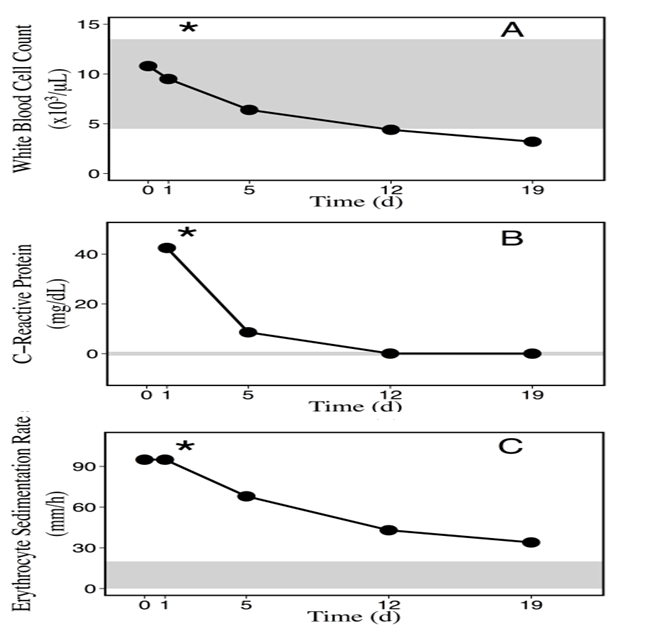
Figure 1: Inflammatory markers decrease over treatment period for intracranial epidural abscess. Grey shading denotes the normal reference ranges for each marker and* indicates neurosurgical intervention.
On admission to our institution, she had a body temperature of 37.2°C, a blood pressure of 112/73 mmHg, a pulse of 100/min, and a respiratory rate of 17/min. She had a Glasgow Coma Score of 15 and a normal neurological examination. Our blood examination of inflammatory markers showed WBC counts of 9.5 x 103/μL, C-reactive protein (CRP) levels of 42.4 mg/L, and an ESR of 95 mm/hr [Figure 1](Time = 1 day). Urine cultures isolated gram-positive flora at 100 CFU/mL while blood cultures at five days showed no growth. All other systems were unremarkable. Notable past medical history included dental surgery at age four.
Neuroimaging
Magnetic resonance (and venogram) imaging (MRI/MRV) studies revealed enhancement of a large bifrontal space-occupying-lesion (SOL), approximately 0.5 cm by 7 cm (long arrow), changes in the frontal sinuses (short arrow), and localized thrombosis involving the anterior aspect of the sagittal sinus Figure 2A, Figure 2C.
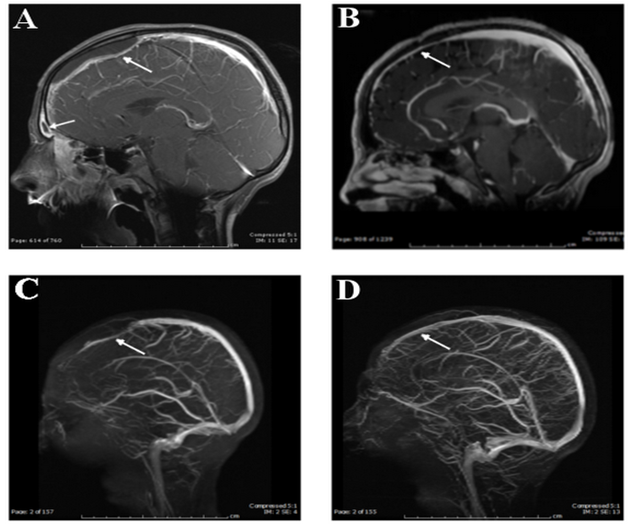
Figure 2: Mild head injury resulting in an epidural abscess and compressed superior sagittal sinus. A large space-occupying lesion is compressing the bifrontal region (A, long arrow) and the anterior aspect of the superior sagittal sinus is attenuated on the MRV (C). Frontal sinus enhancement is also noted (A, short arrow). Resolution of epidural abscess (B, post-op eighteen-months) with decompression of the sagittal sinus as seen on the MRV (D, post-op one-month) following neurosurgical intervention and antibiotic therapy.
Neurosurgical Procedure
Midline frontal burr-hole surgery, with an epicenter nine cm from the glabella, encountered purulent material under pressure Figure 3. Abscess irrigation proceeded with a ventricular catheter passed through the burr-hole, containing a bacitracin solution with added metronidazole, vancomycin, and ceftriaxone.
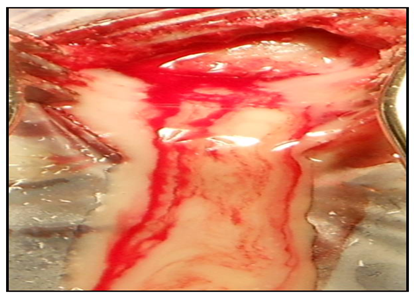
Figure 3: Purulent material of the intracranial epidural abscess encountered at the burr-hole opening.
Post-Operative Course
Abscess cultures isolated Streptococcus intermedius and the patient continued a six-week outpatient intravenous (IV) antibiotic course of ceftriaxone and metronidazole. She tolerated this without incident. Her inflammatory markers decreased [Figure 1] with no further indications of infection. The potential sagittal sinus venous thrombosis complications [Figure 2C] were addressed with a course of dalteparin for 10 days, with dramatic improvement in flow noted at one month [Figure 2D]. Her drainage site healed satisfactory and she was discharged 5 days after surgery. She has remained symptom free at eighteen months. A follow-up MRI at that time demonstrated no abscess recurrence and a patent sagittal sinus [Figure 2B].
Discussion
Intracranial abscesses are oftentimes a difficult diagnosis given the commonality of symptoms, which may include headache and fever (70% - 75%), and less frequently focal neurological deficits (~50%). These symptoms and indicators for infection and inflammatory response, particularly elevated ESR and CRP levels[5,9,10], usually indicate intracranial problems, sometimes arising after traumatic head injury[1,2,4,6,8,11]. Absence of neurological abnormalities in the company of systemic inflammation and infection markers makes the diagnosis and localization of abscesses particularly intricate, as they are often the result of a contiguous focus of infection[2,8]. Our case is an excellent example of these diagnostic challenges. Intracranial problems are an unlikely consideration for the source of infection without symptomatic presentation of focal neurological deficits.
Our patient presented to an outside ED following a minor unwitnessed head injury without loss of consciousness. It is hypothesized that she had an acute epidural hematoma caused by contrecoup head injury by falling backwards off a couch. Epidural hematomas of this nature are rare[12] and may develop without a fracture, because of the increased plasticity of children's bones. The injury causes a separation of the periosteal dura from the calvarium and rupture of the interposed vessels[12]. We speculate that this hematoma became purulent with pathogens seeded from the sinusitis noted on the admit neuroimaging studies or from hematological spread from the UTI. Primary source of infection was never confirmed. Her original symptoms attributed to the UTI (diagnosed with urine cultures positive for Escherichia coli) did not abate during a course of Bactrim therapy, however, urine cultures were negative for growth in our analysis, four days later, likely addressed by the original antibiotic therapy.
Brain abscesses usually begin as an insidious process with non-specific symptoms and minimal neurological abnormalities. Their etiology is commonly attributable to direct extension of contiguous infection (e.g. osteomyelitis of the skull, paranasal sinusitis (Streptococcus pneumonia), middle ear, mastoid or orbit), trauma (Streptococcus aureus), neurosurgical procedures, or hematological spread from a remote focal point[1,4]. Because the infection process here was well contained by the dura, it was unresponsive to the Bactrim therapy and not isolated through blood or urinary analysis. Recognition of the suspected abscess relied exclusively on the imaging studies. Pathogen identification [S. Intermedius] was confirmed via cultures procured from the surgical procedure. It should be noted that the S. Intermedius bacteria is commonly a solitary isolate, only identified by blood culture in one-third of patients[8] and part of the normal flora found in the oral, oropharyngeal, or gastrointestinal areas[13,14]. Current literature suggests that S. Intermedius forming abscesses are deep-seated and associated with hematogenous spread[15], causing purulent infections in the head and neck[13,14,16], central nervous system[13-17], respiratory tract[13], gastrointestinal tract[13], abdominal/pelvic sites[13,14,16,18,19], skin/soft tissues/bones[13,16] and blood[14-16,18,19].
Our case highlights the difficulty and complexity in identifying an intracranial epidural abscess, with probable etiology of acute head injury, and serves as a salient reminder of this rarely seen occurrence. Careful consideration for and review of brain images is paramount in detecting the presence of complications like abscess and venous thrombosis, particularly in case presentations similar to ours[1]. Here, the epidural location explains the persistent cephalgia and fever, unresponsive to Bactrim therapy. Furthermore, the antibiotics, originally prescribed, were directed at E. Coli, rather than the S. Intermedius, which was ultimately cultured from the abscess and addressed with an IV therapy (of ceftriaxone and metronidazole). We suggest that brain abscess should be included in the differential for pediatric and adult patients with a recent history of acute head trauma and prolonged (1 + weeks) symptomatic fever and headaches, with intact neurological function. Furthermore, we suggest that patients who meet this criterion should be worked up for potential intracranial problems, including the use of urinary/blood analysis and imaging studies. The prognosis for treated epidural abscesses are excellent, with most reports[1,4,20,21] indicating a normal recovery.
Acknowledgement: The authors are grateful to the Oregon Research and Education Foundation and the Legacy Foundation Research Fund for supporting this study.
References
- 1. Moonis, G., Granadosa, A., Simon, SL. Epidural hematoma as a complication of sphenoid sinusitis and epidural abscess: a case report and literature review. (2002) Clin Imaging 26(6): 382- 385.
- 2. Tunkel, A. R., Scheld, W. M. Brain Abscess. In: Winn HR. (2011) Youmans Neurological Surgery 588-599.
- 3. Heran, N. S., Steinbok, P., Cochrane, D. D. Conservative Neurosurgical Management of Intracranial Epidural Abscesses in Children. (2003) Neurosurgery 53(4): 893- 897.
- 4. Coyne, T. J., Kemp, R. J. Intracranial epidural abscess: a report of three cases. (1993) Australian and New Zealand journal of surgery 63(2):154- 157.
- 5. Bartt, R. E. Cranial epidural abscess and subdural empyema. (2010) Handbook of clinical neurology 96:75- 89.
- 6. Tsai, Y. D., Chang, W. N., Shen, C.C., et al. Intracranial suppuration: a clinical comparison of subdural empyemas and epidural abscesses. (2003) SurgNeurol 59(3): 191- 196.
- 7. Kaptan, H., Cakiroglu, K., Kasimcan, O., et al. Bilateral frontal epidural abscess. (2008) Neurocirugia (Astur) 19(1): 55- 57.
- 8. Mishra, A. K., Fournier, P. E. The role of Streptococcus intermedius in brain abscess. (2013) Eur J ClinMicrobiol Infect Dis 32(4): 477- 483.
- 9. Kombogiorgas, D, Solanki, G. A. The Pott puffy tumor revisited: neurosurgical implications of this unforgotten entity. Case report and review of the literature. (2006) J Neurosurg 105(2 Suppl): 143- 149.
- 10. Davidson, L., McComb, J. G. Epidural-cutaneous fistula in association with the Pott puffy tumor in an adolescent. Case report. (2006) J Neurosurg 105(3 Suppl): 235- 237.
- 11. Letscher, V., Herbrecht, R., Gaudias, J., et al. Post-traumatic intracranial epidural Aspergillusfumigatus abscess. (1997) Journal of medical and veterinary mycology: bi-monthly publication of the International Society for Human and Animal Mycology 35(4): 279- 282.
- 12. Sato, S., Mitsuyama, T., Ishii, A., et al. An atypical case of head trauma with late onset of contrecoup epidural hematoma, cerebellar contusion, and cerebral infarction in the territory of the recurrent artery of Heubner. (2009) Journal of clinical neuroscience 16(6): 834- 837.
- 13. Whiley, R. A., Beighton, D., Winstanley, T.G., et al. Streptococcus intermedius, Streptococcus constellatus, and Streptococcus anginosus (the Streptococcus milleri group): association with different body sites and clinical infections. (1992) J ClinMicrobiol 30(1): 243- 244.
- 14. Wagner, K. W, Schon, R., Schumacher, M., et al. Case report: brain and liver abscesses caused by oral infection with Streptococcus intermedius. (2006) oral surg oral med oral pathol oral radiolendod 102(4): e21- e23.
- 15. Clarridge, J. E3rd.,Attorri, S., Musher, D. M., et al. Streptococcus intermedius, Streptococcus constellatus, and Streptococcus anginosus ("Streptococcus milleri group") are of different clinical importance and are not equally associated with abscess. (2001) Clin Infect Dis 32(10): 1511-1515.
- 16. Whiley, R. A., Fraser, H. Y., Hardie,J. M., et al. Phenotypic differentiation of Streptococcus intermedius, Streptococcus constellatus, and Streptococcus anginosus strains within the "Streptococcus milleri group". (1990) Journal of clinical microbiology 28(7): 1497- 1501.
- 17. Sommer, D.D., Minet, W, Singh, S. K. Endoscopic transnasal drainage of frontal epidural abscesses. (2011) J otolaryngology head neck surg 40(5): 401- 406.
- 18. Tran, M. P., Caldwell-McMillan, M., Khalife, W., et al. Streptococcusintermedius causing infective endocarditis and abscesses: a report of three cases and review of the literature. (2008) BMC Infect Dis 8: 154.
- 19. Livingston, L. V., Perez-Colon, E. Streptococcus intermedius Bacteremia and Liver Abscess following a Routine Dental Cleaning. (2014) Case Rep Infect Dis 2014: 954046.
- 20. Seto, T., Takesada, H., Matsushita, N., et al. Twelve-year-old girl with intracranial epidural abscess and sphenoiditis. (2014) Brain dev 36(4): 359- 361.
- 21. Kanu, O. O.Ukponmwan, E., Bankole, O., et al. Intracranial epidural abscess of odontogenic origin. (2011) J NeurosurgPediatr 7(3): 311- 315.










