
Intrauterine Treatment of a Fetal Lymphangioma With OK-432 May be not Effective
Jakub Kornacki1*, Michal Blaszczynski2, Jana Skrzypczak1
Affiliation
1 Department of Gynecology, Obstetrics and Gynecological Oncology, Poznan University of Medical Sciences, Poznan, Poland
2 Department of Pediatric Surgery, Traumatology and Urology, Poznan University of Medical Sciences, Poznan, Poland
Corresponding Author
Jakub Kornacki, Division of Reproduction, Department of Gynecology, Obstetrics and Oncology, Pozna? University of Medical Sciences, 3360-535 Pozna?, Poland, Tel: 0048618419302; E-mail: kuba.kornacki@wp.pl
Citation
Kornacki, J., et al. Intrauterine Treatment of a Fetal Lymphangioma With OK-432 May be not Effective. (2018) J Environ Health Sci 4(2): 52- 54.
Copy rights
© 2018 Kornacki, J. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Abstract
We report the case of a fetal neck lymphangioma which was treated antenatally due to an increase in the growth of the lesion. A single intracystic injection of OK-432 was performed at 31 weeks of gestation. The effects of therapy in infant were an increased echogenicity and a slight decrease in the tumor size. The same treatment was continued after the birth, but with a poor response. No complications from antenatal treatment were observed.
Introduction
Case Report
A 28-year old woman was referred to our unit at 27 weeks of gestation because of an ultrasound finding of a fetal neck mass. Ultrasound examination performed in our department confirmed the presence of a poorly vascularized multicystic mass of 4 cm on the anterior of the fetal neck. Based on ultrasound appearance, a lymphangioma was considered. Other fetal anatomical structures and the amniotic fluid volume were normal. Amniocentesis performed during the hospitalization revealed a normal fetal karyotype (46 XY).
Three weeks later, at 30 weeks of gestation, the neck mass size had increased to 7,8 x 6 cm (figure 1). The amount of amniotic fluid remained normal. Because of the significant growth of the mass, intrauterine treatment was undertaken.
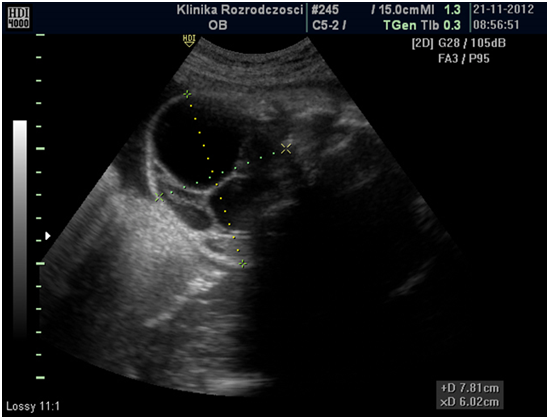
Figure 1: The longitudinal view of the mass at 30 weeks gestation.
At 31 weeks of gestation around 35 ml of fluid was aspirated from the largest fetal neck cyst which was followed by injection of 10 ml of OK-432 (Picibanil) at a concentration of 0,01 mg/ml. To avoid fetal movement during the aspiration and injection the whole procedure was preceded by the direct administration of a muscle relaxation agent into umbilical vein. The intervention was uneventful. One day after the procedure an increased echogenicity of the cyst was noticed. Three weeks later, at 34 weeks, this increased echogenicity of the cystic mass was even more evident (figure 2). At that time, the mass size was 7,3 x 5,7 cm. At 37 weeks of gestation the mass size had decreased to 6,6 x 5,0 cm. Both in ultrasound and in MRI performed at that time there were no signs of fetal airways constriction.
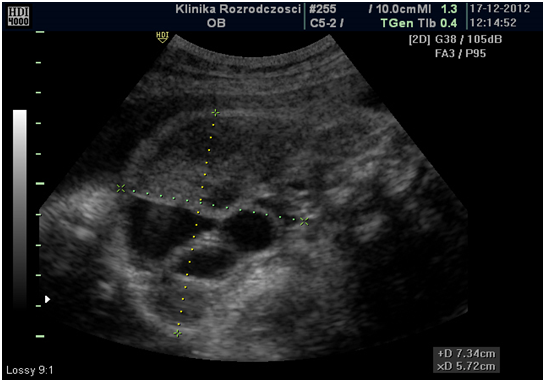
Figure 2: The increased echogenicity of the mass at 34 weeks (3 weeks after injection of OK-432.
At 38 weeks of gestation, a live 3,310 – gram male infant with Apgar score of 7 and 9 at 1 and 5 min, respectively, was delivered by elective caesarean section. A left-sided neck lymphangioma was clinically evident at birth without any airway obstruction (figure 3).

Figure 3: The neck lymphangioma(an image taken on the day a babywas born).
After delivery, constant growth of the mass was observed. The patient was discharged home and scheduled for the sclerotherapy atthe 30th day of life. At this time, ultrasound scans revealed a mixed, macro- and microcystic, structure of the lesion with the largest cyst measuring 4,5 x 1,8 cm. Three procedures of aspiration of the lymph and intracystic injections of OK 432 were performed at the 30th day of life, 3 months and 4,5 months. The volumes of the lymph obtained were 10 cc, 55 cc and 2 cc, the amounts of OK 432 administered were 2 KE, 3 KE and 1 KE, respectively (KE = Klinische Einheit). After sclerotherapies, the signs of inflammatory reactions such as mild fever and flushing were noted with no other local or general symptoms. At a 10 - month follow-up no shrinkage of the lymphangiona was observed. Otherwise, the patient had developed normally. Because of persisting significant deformation of the face patient was subjected to surgical treatment.
Discussion
A differential diagnosis of a fetal neck tumor or cystic lesions include lymphangioma, haemangioma, goiter, neuroblastoma and teratoma (Kornacki, J., et al. 2011). Both ultrasound and magnetic resonance imaging (MRI) enable the differentiation between at least solid or partly solid tumors such as fetal goiter, teratoma or neuroblastoma and cystic or multicystic lesions (lymphangioma, hemangioma).
A diagnosis of a fetal neck lesion is always a serious clinical situation, that may be associated not only with cosmetic consequences for a child but also with life-threatening complications (Kornacki, J., et al. 2011). The most dangerous conditions associated with fetal neck tumors are secondary cardiac failure, typical for large, highly vascularized tumors such as goiter and acute postnatal respiratory distress due to airway compression (Kornacki, J., et al, 2011).
So far, there are no well established methods for the intrauterine treatment of most fetal neck tumors. The most effective one is probably the intra-amniotic therapy of fetal goitrous hypothyroidism with repeated intrauterine injections of L-thyroxine (Ribault, V., et al, 2009; Kornacki, J., et al. 2011).
Another, more controversial method for the intrauterine treatment of fetal neck lesions, which is restricted to lymphangioma, is the intracystic injection of OK-432.
OK-432 is a sclerotherapy agent that was used for the first time in the postnatal treatment of a neck lymphangioma in 1987 (Ogita, S., et al. 1994). It is a lyophilized mixture of low-virulence group A Streptococcus pyogenes Su strain bacteria incubated with a low concentration of benzyl penicillin (Ogita, S, et al, 1996). The exact mechanism of its action is unknown, but the effectiveness of the drug is probably the consequence of its proinflammatory activity, including increased productions of various cytokines (Yang, K.D., et al. 1992; Narkio-Makela, M., et al. 2011).
So far, there is only one case report on the successful intrauterine therapy of a fetal neck lymphangioma by intracystic injection of OK-432(Mikovic, Z., et al. 2009). The authors of this study described an almost complete disappearance of the lesions after single injections of OK-432 in two fetuses.
In comparison to the single study of the antenatal therapy of a neck lymphangioma with OK-432, postnatal treatment is widely used and accepted (Yoo, J.C., et al., 2009; Narkio-Makela, M., et al. 2011; Kim, D.W., 2014;). It became an effective and popular alternative to surgical treatment, and often more preferable to surgery because of its safety (Narkio-Makela, M., et al. 2011). The effectiveness of postnatal therapy after a single or repeated injection of OK-432, as reported by different authors, is around 70 - 80% (Yoo, J.C., et al., 2009; Kim, D.W., 2014) .
The two remaining reports on the antenatal use of OK-432 concern the rescue treatment of fetal chylothorax (Tanemura, M., et al. 2001; Lo, T.K., et al. 2012). In both studies, the authors observed a resolution of the fetal chylothorax after a single or repeated intra thoracic injections of OK-432.
In the clinical case presented by us, in comparison to the two cases described by Mikovic et al. (2009), we did not observe a resolution of the lesion after a single injection of OK-432. The only positive effect we observed was a slight and transient decrease in tumor size. We do not know if this had any clinical significance, including the decreased risk of fetal airway obstruction.
More interestingly, no sufficient therapeutic effect was observed after the postnatal therapy. The reason for this may be the mixed, mostly microcystic character of the mass. In several studies the microcystic lesions were significantly more resistant to sclerotherapy with OK-432 than macrocystic one (Banieghbal, B., et al. 2003; Luzzatto, C., et al. 2005; Narkio-Makela, M., et al. 2011).
In microcystic lymphangioma, the access of drugs to cysts may be difficult and the connective tissue surrounding cysts makes the shrinkage of mass less effective (Banieghbal, B., et al. 2003; Luzzatto, C., et al. 2005).
Conclusion
Despite the fact that lymphangioma may often not compress the fetal airways and this is why the anetanatal treatment is controversial, the very big, rapidly growing massess may theoretically cause postnatal acute respiratory failure of the fetus which life threating condition. In the experienced hands, the intaruterine therapy, if undertaken, is rather not asscoiated with high complications rate and this is why may be eventually considered.
Conflicts of Interest: None.
References
- 1. Banieghbal, B., Davies, M.R. Guidelines for the successful treatment of lymphangioma with OK-432. (2003) Eur J Pediatr Surg 13(2): 103-107.
- 2. Kim, D.W. OK-432 sclerotherapy of lymphatic malformation in the head and neck; factors related to outcome. (2014) Pediatr Radiol 44(7): 857-862.
- 3. Kornacki, J., Mroziński, B., Skrzypczak, J. A rare case of recurrent fetal goiter. (2011) Fetal Diagn Ther 31(1): 69-72.
- 4. Lo, T.K., Lau, W.L., Tang, M.H.Y., et al. Successful treatment of severe fetal chylothorax resistant to repeated pleuroamniotic shunting by OK-432 pleurodesis. (2012) Fetal Diagn Ther 31(4): 260-263.
- 5. Luzzatto, C., Lo Piccolo, R., Fascetti Leon, F., et al. Further experience with OK-432 for lymphangiomas. (2005) Pediatr Surg Int 21(12): 969-972.
- 6. Mikovic, Z., Simic, R., Egic, A., et al. Intrauterine tretament of large fetal neck lymphangioma with OK-432. (2009) Fetal Diagn Ther 26(2): 102-106.
- 7. Narkio-Makela, M., Makela, T., Saarinen, P., et al. Treatment of lymphatic malformations of head and neck with OK-432 sclerotherapy induce systemic inflammatory response. (2011) Eur Arch Otorhinolaryngol 268(1): 123-129.
- 8. Ogita, S., Tsuoto, T., Nakamura, K., et al. OK-432 therapy in 64 patients with Lymphangioma. (1994) J Pediatr Surg 29(6): 784-785.
- 9. Ogita, S., Tsuoto, T., Nakamura, K., et al. OK-432 therapy for lymphangioma in children: why and how does it work? (1996) J Pediatr Surg 31(4): 477-480.
- 10. Ribault, V., Castanet, M., Bertrand, A.M., et al. French Fetal Goiter Study Group: Experience with intra amniotic thyroxine treatment in Nonimmune fetal goitrous hypothyroidism in 12 cases. (2009) J Clin Endocrinol Metab 94(10): 3731- 3793.
- 11. Tanemura, M., Nishikawa, N., Kojima, K., et al. A case of successfull fetal Therapy for congenital chylothorax by intrapleural injection of OK-432. (2001) Ultrasound Obstet Gynecol 18(4): 371-375.
- 12. Yang, K.D., Stone, R.M., Lee, C.S., et al. Effect of picibanil (OK-432) on neutrophil-mediated antitumor activity: implication of monocyte-derived neutrophil-activating factors. (1992) Cancer Immunol Immunother 35(4): 277-282.
- 13. Yoo, J.C., Ahn, Y., Lim, Y.S., et al. OK-432 sclerotherapy in head and neck lymphangiomas: Long-term follow-up result. (2009) Otolaryngol Head Neck Surg 140(1): 120-123.










