
Surface Area of the Prosthesis Support Polygon with Different Implant Configurations in Edentulous Maxillae
Wentaschek S*, Seiß S, Igiel C, Behneke N
Affiliation
Department of Prosthetic Dentistry, University Medical Center of the University of Mainz, Augustusplatz, Mainz, Germany
Corresponding Author
Stefan Wentaschek, DMD, MSc. Department of Prosthetic Dentistry, University Medical Center of the University of Mainz, Augustusplatz 2, 55131 Mainz, Germany, Tel: +49-6131 17 3062/ Fax: +49-6131 17 5517; E-mail: stefan.wentaschek@unimedizin-mainz.de
Citation
Wentaschek, S., et al. Minimally Invasive Dentistry Approach Benefits of Using Laser. (2017) J Dent Oral Care 3(1): 1- 4.
Copy rights
© 2017 Wentaschek, S. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
In vitro study; Tilted implants; Edentulous maxilla; Surface area of prosthesis support
Abstract
Background: A minimum of four implants should be used in edentulous maxillae to anchor a dental prosthesis. A wide anterior/posterior distribution of the implants is advantageous. Besides bone grafting, short or tilted implants are used to achieve this in atrophic edentulous maxillae. The implants define a polygon that should be as large as possible. This study investigated the differences in the surface area of the polygon of implant-retained prosthesis support with straight and tilted dental implants in edentulous maxillae.
Materials and Methods: In fifty DICOM-datasets of atrophic edentulous maxillae, four different implant configurations using four implants each were virtually planned and measured. The distal implants were either straight (12, 10 or 8 mm long) or tilted (≥ 12 mm) and positioned as distally as possible without bone grafting.
Results: The mean surface area of the prosthesis support polygon with straight implants distally, 12 mm in length, was 263 mm² (SD: 134, range: 36 to 590 mm²). The use of 2 mm shorter implants resulted in an enlargement of the support polygon of about 20 %. By using tilted implants (42 to 45°), the size of the polygon (mean: 456 mm², SD: 180, range: 151 to 949 mm²) was increased by another 20 % compared to straight 8 mm long implants.
Conclusion: This study demonstrated that the implant-retained prosthesis support area can be enlarged by reducing the implant length of distal implants, and it can be further enlarged in edentulous maxillae by using tilted implants.
Introduction
At the beginning of today’s common dental implantology, only edentulous patients were treated with implants and they have always been treated with fixed superstructures[1]. At this time, the placement of fixtures should be limited to the area between the mental foramina in the mandible and between the anterior sinus recesses in the upper jaw. Cantilevered extensions have been used to provide an adequate replacement of dentition[1]. The 10-year implant survival rate in the upper jaw was lower than in the mandible which was, among other things, attributed to the small available bone volume between the sometimes expanded maxillary sinus recesses followed by too long distal cantilever extensions[2]. In the course of time, various methods to treat edentulous jaws without accepting too large cantilever extensions were established. This includes, inter alia, the implantation in previously grafted bone to enable a more distal position of the implants. Nowadays, sinus floor elevation, prior to implantation, is a clinically valid therapeutic method[3]. Nevertheless, augmentation procedure could be associated with various additional complications such as morbidity in the donor region, sinusitis, loss of the augmentation material, unpredictable absorption and osteomyelitis[4]. Augmentation procedure is challenging for the dentist as well as for the patient and, in addition to the increased surgical risks, it is often associated with an extension of treatment time and increasing costs[5]. Another method to insert implants in areas with reduced bone volume without bone grafting, is the use of short implants with an intra osseous length of less than 8 mm[5]. But short implants might be inferior in immediate loading protocols where a high primary stability is important[6].
The idea arose to increase the polygon of implant retained prostheses support by tilting the distal implants along the anterior wall of the maxillary sinus, and thereby allowing a more posterior supported denture[7]. Originally, surgery was done under direct vision after fenestration of the maxillary sinus. This technique seems to have high expectations and finds a further distribution since the establishment of the guided 3D planned implantation[5]. The aim is placing implants of conventional length, increasing the polygonal area of prosthesis support and reducing the cantilever length. Instead of using tilted implants, these regions would receive shorter implants[5]. To that effect, the increase of inter-implant distance using tilted implants depends on the alternatively used implant length.
Because the mean enlargement of the support polygon with tilted implants compared to straight implants is unknown, the aim of this study was to evaluate the increase of the surface area of this polygon, which results from the use of tilted distal implants in comparison to straight implants with different lengths in the edentulous maxilla.
Materials and Methods
DICOM-datasets of 50 atrophic edentulous maxillae were analyzed (28 women, 22 men, mean age: 61.6 years [range: 39 to 82 years; standard deviation (SD): 9.7 years]). Posterior ridge dimension of all maxillae would not allow the placement of an implant with an intra osseous length of at least 8 mm without bone grafting in the molar region.
All anonymized cone-beam computed tomography (CBCT) data were consecutively selected with the same inclusion criteria as described earlier[8].
In the 50 DICOM-datasets two reference implants were virtually positioned in the maxillary lateral incisor region (SKYplanX, Bredent) and two straight 12 mm (group 1), 10 mm (group 2) and 8 mm (group 3) implants were virtually positioned distally to those. In Group 4, two distally tilted implants of 12 to 16 mm with an inclination of 42 to 45° were positioned. Each implant was positioned as distally as possible without bone grafting (Figure 1).
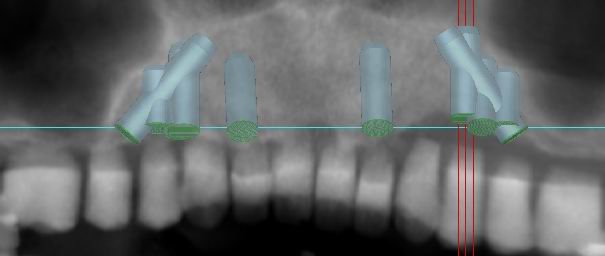
Figure 1: Virtually positioned straight implants 12, 10 and 8 mm in lengths and tilted implants 16 mm in lengths distal and two reference implants between them.
With the validated measuring tool of the 3D planning software, the differences in the polygonal prostheses support areas were measured in the sagittal and transversal distance as well as the polygon diagonals and the angle between them to calculate calculate the plane of the convex quadrilateral defined by the four implants for all four groups ([1] straight, 12 mm; [2] straight, 10 mm; [3] straight, 8 mm; [4] tilted, 12 - 16 mm) (Figure 2).
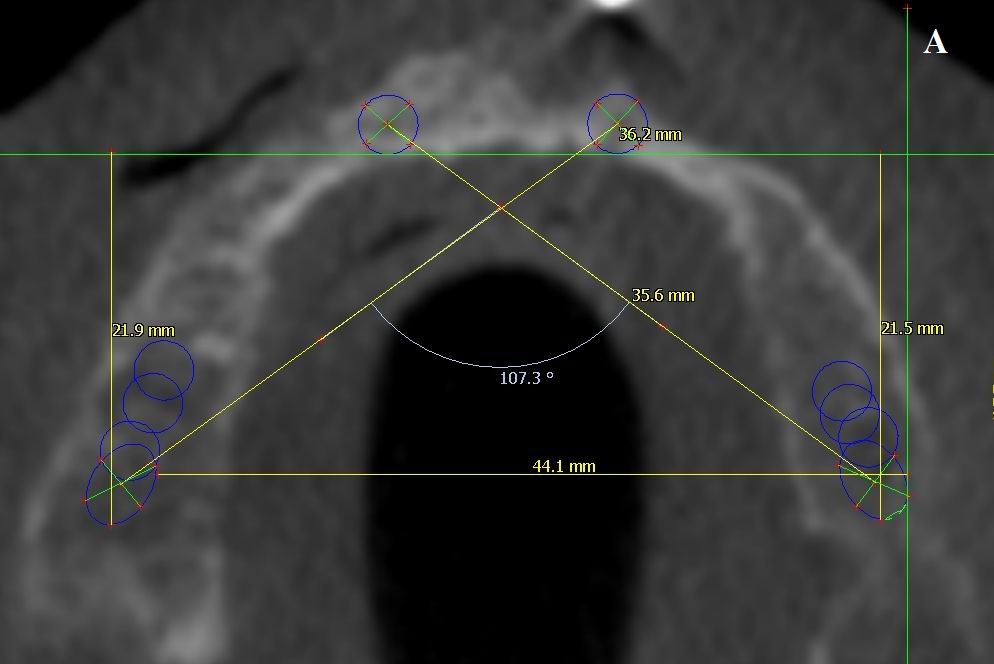
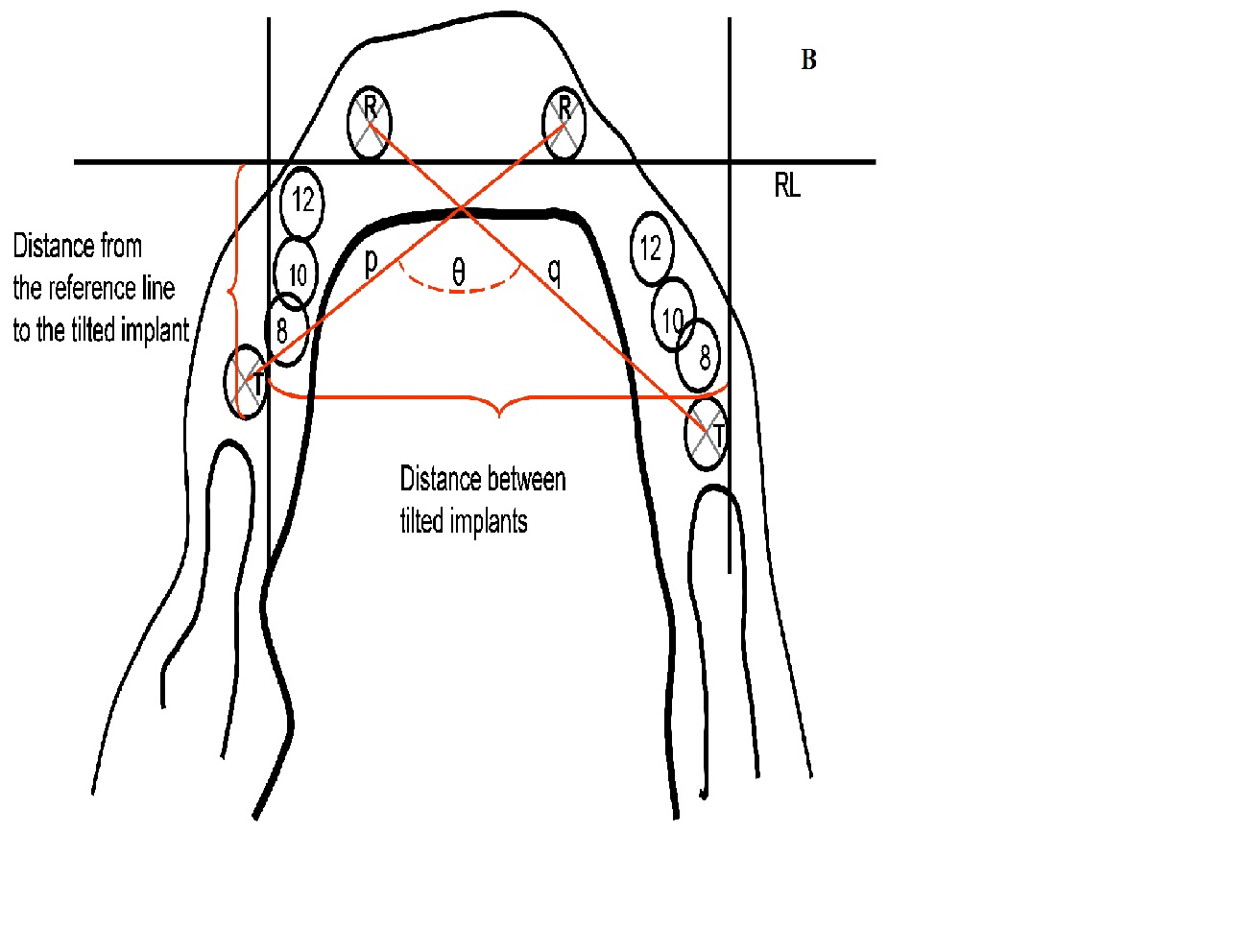
Figure 2: Occlusal view of the implant positions and the measurement technique in screenshot (a) and diagram (b). R = reference implant; 12 = 12 mm implant; 10 = 10 mm implant; 8 = 8 mm implant; T = tilted implant; RL = reference line; p and q = polygon diagonals; θ = angle between polygon diagonals.
Statistical analysis
Statistical analysis was performed with the SPSS 15.0 (SPSS Inc., Chicago, USA) program.
The patient-related differences between the four different plans always changed in the same direction. Consequently, mean comparisons always result in a significant difference. Therefore, the results of four different plans for each patient were only examined by descriptive statistics.
Results
Lengths and angles of inclination for the angulated distal implants are present in table 1.
The mean transversal distance between the reference implants was 15.1 mm (SD: 3.9, range: 6.9 to 29.7 mm) and 33.9 mm (SD: 5.1, range: 16.7 to 43.4 mm) for the two distal implants in group 1, 35.3 mm (SD: 4.9, range: 19.8 to 44.3 mm) for group 2, 37.0 mm (SD: 4.8, range: 21.8 to 46.9 mm) for group 3 and 39.4 mm (SD: 4.6, range: 27.6 to 50.7 mm) for group 4.
Table 1: Implant lengths and insertion angles for the angulated distal implants of group 4.
| N | Mean | SD | 95% | Minmum | Maximum | ||
|---|---|---|---|---|---|---|---|
| Lower bound | Upper bond | ||||||
| Implant length tilted right (mm) | 50 | 15.4 | 1.1 | 15.1 | 15.7 | 12.0 | 16.0 |
| Implant length tilted left (mm) | 50 | 15.3 | 1.2 | 14.9 | 15.6 | 12.0 | 16.0 |
| Angle, titled right (°) | 50 | 43.9 | 1.2 | 43.6 | 44.3 | 42 | 45 |
| Angle, titled left (°) | 50 | 44.1 | 1.2 | 43.7 | 44.4 | 42 | 45 |
The measured sagittal depths of the implant-retained prosthesis support polygons are shown in Figure 3.
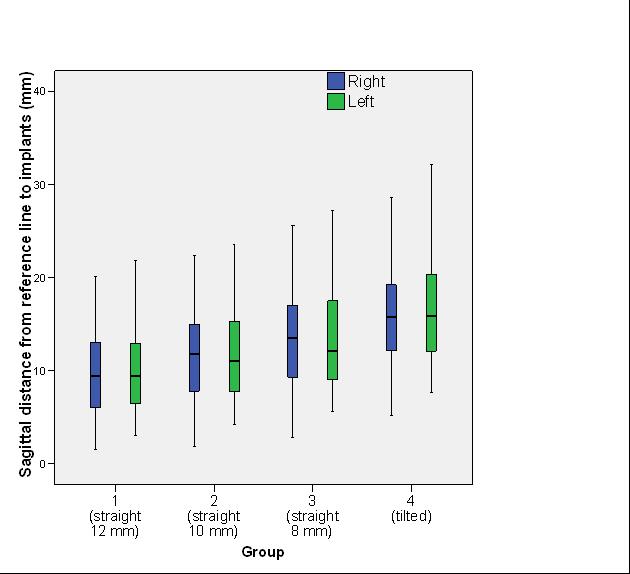
Figure 3: Box plot represent the mesio-distal distance from the reference line to the different distal implants.
The calculated surface areas of the convex quadrilateral that are spanned by four implants of the support polygons are shown in Figure 4.
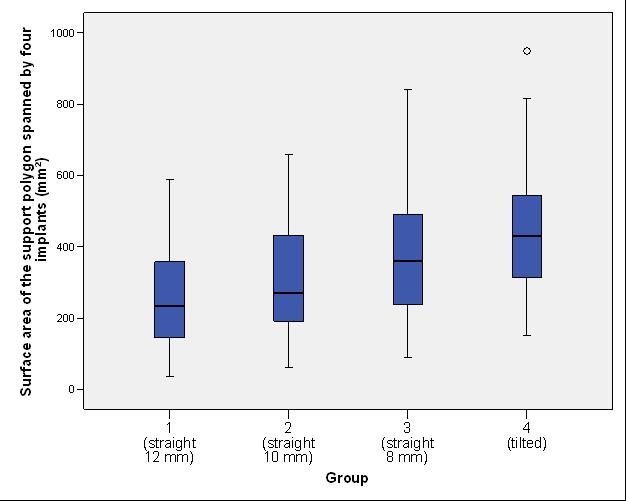
Figure 4: Box plot represent the surface area of the support polygons for groups 1, 2, 3 and 4.
Discussion
In the present study, the approximate mean surface area of the prosthesis support polygon in group 1 was 265 mm2; 315 mm² in group 2; 375 mm² in group 3 and 455 mm² in group 4, respectively. The difference between tilted implants (in mean 15 mm in length) compared to straight implants 8 mm in length represents an increase of about 20%. Between straight implants 12 mm and 10 mm in length and between 10 mm and 8 mm in length the difference was also about 20%. The mean sagittal depth of the supported polygon in group 1 was approximately 10 mm and the corresponding differences in the depth of the support polygon between the four groups were in an average of 15 to 20%. The differences in the depth of the supported polygon differ from other investigations. In an in vivo study a mean increase of about 9 mm of the maxillary implant support area with an implant angulation of 30 to 35° was reported[9]. With a lower inclination this exceeds the results of this study by 50% in comparison of group 1 and 4 where the enlargement was about 6 mm. In that study, distances were measured on a 2-dimensional orthopantomogram. Analyzed was the mesio-distal distance from the point at which the tilted implant supported the prosthesis to the point at which an upright implant in the same patient would have provided support. In cases in which the patient had sufficient bone posterior to the maxillary sinuses, the authors also inserted anteriorly tilted implants and that can explain the difference[9].
In various studies, it was shown that the enlargement of the support polygon with tilted implants can lead to a significant reduction of biomechanical stresses around implant supported prosthesis[10,11]. Bevilacqua et al. used 3D finite element analysis to compare the load transfer to the peri-implant bone in the edentulous jaw for implants that were inserted angulated versus vertically to the occlusal plane. The authors held the prosthesis length constant and evaluated four different configurations with four implants each and with the distal implants inclined at 0°, 15°, 30°, and 45°. The greater the inclination, the shorter the resulting cantilever extensions: 15, 11.6, 8.3, and 5 mm, respectively. A vertical load of 150 N was applied to the distal portion of the posterior cantilevers. The authors recorded the maximum stresses in the peri-implant bone of the distal and mesial implants and in the metal framework. In cancellous bone, the three parameters decreased by 56%, 55.5% and 42.3% for the 45° configuration; 47.6%, 48.1% and 23.6% for the 30° configuration; 17%, 33.3% and 10.9% for the 15° configuration, respectively, with a consequent reduction in the posterior cantilevers, compared with the vertical implants[11].
Although there is a lack of randomized studies, the angulationof implants to the occlusal plane, and thus their extra-axial loading during chewing, do not appear to lead to mechanical or biological complications[12,13]; furthermore, according to the literature, there seems to be no clinically relevant negative impact on the implant survival rate or on the peri-implant bone loss in the upper jaw[13]. Therefore, considering the literature data and the results of this study, the use of tilted implants in edentulous maxillae appears to be a valid therapeutic alternative to implant-supported prostheses supported by straight implants.
Conclusion
The use of shorter implants in edentulous maxillae can increase the prosthesis support polygon by 20 % for every two millimeters saved in the used implant length (between 12 and 8 mm). By using tilted implants (42 to 45°, 12 to 16 mm in length) the support polygon can be increased by another 20 % compared to non-tilted 8 mm implants. Considering the results of this study, the use of tilted implants in edentulous maxillae appears to be a therapeutic alternative to shorter implants in the molar region if bone grafting needs to be avoided.
Acknowledge:
The authors would like to thank Bredent Medical (Senden, Germany) for providing the 3D planning system free of charge.
Conflict of interest:
The authors report no conflict of interest related to this study.
References
- 1. Branemark, P.I. Osseointegration and its experimental background. (1983) J Prosthet Dent 50(3): 399-410.
- 2. Adell, R., Eriksson, B., Lekholm, U., et al. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. (1990) Int J Oral Maxillofac Implants 5(4): 347-359.
- 3. Jensen, S.S., Terheyden, H. Bone augmentation procedures in localized defects in the alveolar ridge: clinical results with different bone grafts and bone-substitute materials. (2009) Int J Oral Maxillofac Implants 24(Suppl): 218-236.
- 4. Aparicio, C., Perales, P., Rangert, B. Tilted implants as an alternative to maxillary sinus grafting: a clinical, radiologic, and periotest study. (2001) Clin Implant Dent Relat Res 3(1): 39-49.
- 5. Del Fabbro, M., Bellini, C.M., Romeo, D., et al. Tilted Implants for the Rehabilitation of Edentulous Jaws: A Systematic Review. (2012) Clin Implant Dent Relat Res 14(4): 612-621.
- 6. Papaspyridakos, P., Chen, C.J., Chuang, S.K., et al. Implant loading protocols for edentulous patients with fixed prostheses: a systematic review and meta-analysis. (2014) Int J Oral Maxillofac Implants 29(Suppl): 256-270.
- 7. Mattsson, T., Kondell, P.A., Gynther, G.W., et al. Implant treatment without bone grafting in severely resorbed edentulous maxillae. (1999) J Oral Maxillofac Surg 57(3): 281-287.
- 8. Wentaschek, S., Lehmann, K.M., Scheller, H., et al. Polygonal Area of Prosthesis Support with Straight and Tilted Dental Implants in Edentulous Maxillae. (2016) Int J Prosthodont 29(3): 245-252.
- 9. Krekmanov, L., Kahn, M., Rangert, B., et al. Tilting of posterior mandibular and maxillary implants for improved prosthesis support. (2000) Int J Oral Maxillofac Implants 15(3): 405-414.
- 10. Bellini, C.M., Romeo, D., Galbusera, F., et al. A finite element analysis of tilted versus nontilted implant configurations in the edentulous maxilla. (2009) Int J Prosthodont 22(2): 155-157.
- 11. Bevilacqua, M., Tealdo, T., Pera, F., et al. Three-dimensional finite element analysis of load transmission using different implant inclinations and cantilever lengths. (2008) Int J Prosthodont 21(6): 539-542.
- 12. Monje, A., Chan, H.L., Suarez, F., et al. Marginal bone loss around tilted implants in comparison to straight implants: a meta-analysis. (2012) Int J Oral Maxillofac Implants 27(6): 1576-1583.
- 13. Chrcanovic, B.R., Albrektsson, T., Wennerberg, A. Tilted versus axially placed dental implants: A meta-analysis. (2014) J Dent 43(2): 149-170.










