
The Efficacy of Three Different Doses of Intrathecal Fentanyl for Prevention of Shivering in Lower Limb Orthopedic Surgeries: A Randomized Double-Blind Controlled Trial
Mohammadreza Safavi1, Azim Honarmand1*, Tina Foodeh1, Seyed Mohammad Amin Nourian1, Masoud Nazem2, Daruosh Moradi1, Shahnaze Barvarz1
Affiliation
- 1Department of Anesthesiology and Critical Care Research Center, Isfahan University of Medical Sciences, Isfahan, Iran
- 1Department of Pediatric Surgery, Isfahan University of Medical Sciences, Isfahan, Iran
Corresponding Author
Azim Honarmand, Professor , Department of Anesthesiology and Critical Care Research Center, Isfahan University of Medical Sciences, Isfahan, Iran, Tel:0989133136286; E-mail: honarmand@med.mui.ac.ir
Citation
Honarmand, A., et al. The Efficacy of Three Different Doses of Intrathecal Fentanyl for Prevention of Shivering in Lower Limb Orthopedic Surgeries: A Randomized Double-Blind Controlled Trial. (2016) J Anesth Surg 3(2): 153-158.
Copy rights
© 2016 Honarmand, A. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Shivering; Fentanyl; Anesthesia, Spinal; Bupivacaine
Abstract
Background: Fentanyl has been used to prevent shivering in spinal anesthesia but still the effects of different doses have not been appropriately specified. The aim of this study was to assess the effect of 10 μg, 20 μg and 30 μg intrathecal fentanyl on prevention of shivering during and after lower limb orthopedic surgeries under spinal anesthesia.
Materials and Methods: One hundred and twenty patients undergoing elective orthopedic surgery under spinal anesthesia were enrolled in this clinical trial. Subjects were randomly divided to four groups; Group P received 3 cc bupivacaine 0.5% plus normal saline intrathecally; Group A10 received 10 μg fentanyl plus 3 cc bupivacaine 0.5% intrathecally; Group B20 received 20 μg fentanyl plus 3 cc bupivacaine 0.5% intrathecally; and Group C30 received 30 μg fentanyl plus 3 cc bupivacaine 0.5% intrathecally. Shivering and the complications were recorded. Results: Shivering intensity was different between 4 groups (P = 0.014). There was no moderate, severe and very severe shivering seen in Group C30 but there was 16.7% moderate, 10% sever, and 6.7% very severe shivering seen in Group P. The total incidence of shivering after spinal anesthesia in Groups A10, Group B20, Group C30 and Group P were 53.5%, 26.7% , 6.7% and 63.3% respectively and there was statistically significant difference between 4 group in this regard (P < 0.001).
Conclusion: Intrathecal bupivacaine combined with 30 μg fentanyl was superior to using 10 μg or 20 μg fentanyl for prevention of shivering during lower extremity orthopedic surgery.
Introduction
Shivering is one of the common problems after spinal anesthesia with an incidence of up to 56.7%[1-3]. It increases oxygen consumption, lactic acidosis, carbon dioxide production and catecholamine release[4-7].
One of the primary causes of post anesthesia shivering (PAS) is hypothermia which is due to direct inhibition of body thermoregulatory mechanisms by anesthetics, decreased metabolism, patient’s exposure to cold environment of operating rooms and body cavity exposure[8].
Shivering, along with pain, nausea and vomiting are cases of discomfort and dissatisfaction in patients undergoing spinal anesthesia[9].
The combination of lipophilic opioids with hyperbaric bupivacaine during spinal anesthesia provides reduced latency, longer duration of anesthesia and better quality of anesthesia[10]. Another known effect of intrathecal opioids is prevention and treatment of postoperative shivering[11].
Fentanyl is well known for its rapid onset and shorter duration of action following intratechal administration[12,13]. Small doses of fentanyl (10 - 40 μg) administered directly into the cerebrospinal fluid has been found to be very effective in minimizing discomfort during cesarean delivery without increasing serious adverse effects[13-17]. Chow et al[18] showed that low dose intratechal fentanyl during transurethral resection of prostate (TURP) under spinal anesthesia was an effective method for decreasing both the incidence and intensity of shivering.
Other studies performed by Techanivate et al[19,20] showed the incidence of shivering after appendectomy and cesarean delivery was significantly lower in fentanyl group when compared with saline normal which was added to bupivacaine or mixture of bupivacaine and morphine.
To the best of our knowledge there was no previous study to evaluate various intratechal fentanyl doses on prevention of intraoperative shivering during spinal anesthesia in non-pregnant patients. So we designed the present study to assess the effect of 10 μg, 20 μg and 30 μg intratechal fentanyl on prevention of shivering during and after lower limb orthopedic surgeries.
Materials and Methods
After obtaining institutional approval from the Ethic Committee of University and taking informed consent from the patients, 120 American Society of Anesthesiologists (ASA) physical statuses I – II patients scheduled for elective lower limb orthopedic surgery under spinal anesthesia were included in this double blinded randomized clinical trial study. Other inclusion criteria were as follows: age ranged from 18 to 65 years, lack of previous history of Convulsion, Psychological disease, Hypertension, Hyperthyroidism, Cardiopulmonary disease, Alcoholism, Vasodilator using and lack of fever, Hypothermia or Bleeding tendency and Allergy to the local anesthetics or fentanyl, Metoclopramide, Ephedrine and Pethidine. Exclusion criteria were any change in anesthesia technique and need to the intra-operative blood transfusion.
Before the study was begun, a random table was used to generate a randomized schedule specifying the group to which each patient would be assigned up on entry into the trial. In case of exclusion, the next patient was randomized per schedule. The included patients were divided into four groups each with 30 members. The patients in the first group (Group A10) received 10μg fentanyl plus 3 cc bupivacaine 0.5% intratechally; the second group (Group B20) received 20 μg fentanyl plus 3cc bupivacaine 0.5%; the 3rd group (Group C30) received 30 μg fentanyl plus 3cc Bupivacaine; and the fourth group (Group P) received 3cc bupivacaine 0.5% plus normal saline.
All drugs were diluted with sterile normal saline to give 5 ml solutions, which were administered intrathecally. Also all drugs were labeled with the randomization number of the patient. Patients and staff involved in data collections were unaware of the patient group assignment. Spinal anesthesia was done with quince spinal needle number 25 at L2 – L4 level in the sitting position. A wide bore intravenous catheter (no: 18) into a forearm vein was inserted and ringer lactate 10 ml/kg was administered. Monitoring were included oral and tympanic temperature, pulse oximetry, noninvasive arterial blood pressure and ECG.
Core and peripheral body temperature were recorded every 15minutes by tympanic and oral thermometer respectively intraoperative and during recovery period. The ambient temperature was hold at 22 - 24°C and 25 - 27°C intra-operatively and in recovery room respectively. Infused fluids were warmed up to environmental temperature.
Sensory analgesia was evaluated by pinprick before the start of surgery and re checked for at least 15 minute after spinal anesthesia. Mean arterial blood pressure and heart rates were recorded every 15 minutes with noninvasive blood pressure monitoring and pulse oximetry. Shivering involving whole body was checked every 5minutes during surgery and at recovery room by a 4 point rating score system (0: none, 1: mild fasciculation in face or neck, 2: visible tremor in more than one muscle group, 3: shivering involving whole body) for 2 hours[6,7,19,20]. In case of shivering score ≥ 2 intravenous pethidine 0.5 mg/kg was given.
Perioperative hypotension, bradycardia, Nausea, and vomiting were assessed. Bolus of fluid or incremental doses of ephedrine 10 mg IV was used to treat hypotension (SBP < 30% from baseline or < 80 mmHg), and intravenous Atropine 0.5 mg used to treat bradycardia (HR < 40 bpm or HR < 60 with hypotension). Pain was checked objectively at the time of patient complain by visual analogue scale (0: None, 10 = the worst imaginable pain) and pain with VAS ≥ 4 was treated with incremented dose of fentanyl 25 μg IV. Nausea and vomiting was managed with metoclopromide 0.15 mg/gr IV as necessary. A sample of 120 patients (4 groups of 30) was calculated to be required with standard errors of 0.05, a power of 0.95 and d = 1.2 based on previous relevant clinical data. Statistical analysis was performed with SPSS version 22 software using chi-square, ANOVA and Man-Whitney tests.
Results
We performed a double blind, prospective, randomized study to determine the preventive effects of various low doses of intratechal fentanyl on shivering in elective lower limb orthopedic surgeries under spinal anesthesia.
A total of 120 patients were studied. The four study groups were comparable with respect to age, sex, weight, highest sensory level, type and duration of surgery and ASA functional Class [Table 1].
Table 1: Demographic data of patients, type and duration of surgery and maximum sensory level 1 in 4 groups (Mean ± SD or n-%)
| Variable group | Group P | Group 10 | Group 20 | Group 30 | P | |
|---|---|---|---|---|---|---|
| Age (year) | 38 ± 13.2 | 42 ± 15.3 | 42.7 ± 15.1 | 39.4 ± 15.1 | 0.58 | |
| Weight (Kg) | 66.8 ± 9.6 | 66.1 ± 8.4 | 66 ± 11.7 | 69.6 ± 10.4 | 0.48 | |
| Operation time (min) | 39.7 ± 20.2 | 93.9 ± 17.9 | 96.2 ± 18.5 | 94.9 ± 18.3 | 0.91 | |
| Sex (n-%) | Male | 16 (53.3) | 17 (56.7) | 15 (50) | 15 (50) | 0.95 |
| Female | 14 (46.7) | 13 (43.3) | 15 (50) | 15 (50) | ||
| ASA (n-%) | I | 18 (60) | 17 (56.7) | 16 (53.3) | 15 (50) | 0.88 |
| II | 12 (40) | 13 (43.3) | 14 (46.7) | 15 (50) | ||
| Type of surgery (n- %) | DHS | 5 (16.7) | 6 (20) | 4 (13.3) | 5 (16.7) | 0.92 |
| Femur | 4 (13.3) | 8 (26.7) | 8 (26.7) | 3 (10) | ||
| Knee | 8 (26.7) | 6 (20) | 6 (20) | 9 (30) | ||
| Tibia | 8 (26.7) | 6 (20) | 6 (20) | 8 (26.7) | ||
| Ankle | 5 (16.7) | 4 (13.3) | 6 (20) | 5 (16.7) | ||
| Maximum sensory level | 6 | 6 (20) | 5 (16.7) | 5 (16.7) | 5 (16.7) | 0.99 |
| 7 | 8 (26.7) | 7 (23.3) | 11 (30.7) | 8 (26.7) | ||
| 8 | 9 (30) | 8 (26.7) | 8 (26.7) | 8 (26.7) | ||
| 9 | 4 (13.3) | 6 (20) | 3 (10) | 5 (16.7) | ||
| 10 | 3 (10) | 4 (13.3) | 3 (10) | 4 (13.3) | ||
As is shown in Figure 1 the total incidence of shivering after spinal anesthesia in groups 10, 20, 30 and P were 53.5%, 26.7% , 6.7% and 63.3% respectively and according to chi – square test there was statistically significant difference between 4 group in this regard (P < 0.001).
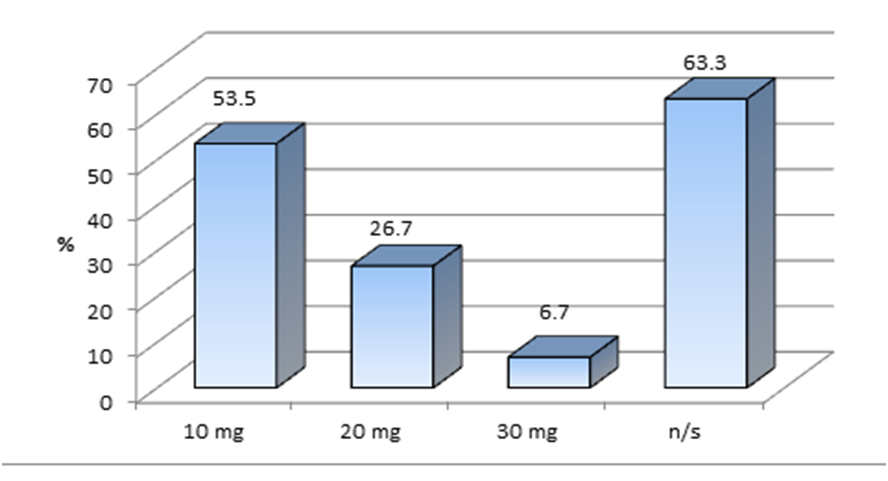
Figure 1: Frequency and incidence of postoperative shivering in 4 groups.
Shivering intensity was different between 4 groups (p = 0.014). According to Table 2 no moderate, severe and very severe chills was seen in group 30, but there was 16.7% moderate 10% sever and 6.7% very chills seen in group P.
Table 2: Frequency of shivering intensity in 4 groups (n- %)
| Group Shivering intensity | Group P | Group 10 | Group 20 | Group 30 |
|---|---|---|---|---|
| No shivering | 11 (36.7) | 14 (46.4) | 22 (73.3) | 28 (93.3) |
| Mild shivering | 9 (30) | 4 (13.3) | 5 (16.7) | 2 (6.7) |
| Moderate shivering | 5 (16.7) | 4 (23.3) | 2 (6.7) | 0 (0) |
| Severe shivering | 3 (10) | 3 (10) | 1 (3.3) | 0 (0) |
| Very severe shivering | 2 (6.7) | 2 (6.7) | 0 (0) | 0 (0) |
P = 0.04
As shown in Table 3 there was no significant difference between group P and group 10 in regard to incidence and severity of shivering but this is significant between other groups when compared with each other.
Table 3: Intensity and incidence of shivering between groups (P value comparison)
| Group P | Group 10 | Group 20 | Group 30 | |||||
|---|---|---|---|---|---|---|---|---|
| Intensity | Incidence | Intensity | Incidence | Intensity | Incidence | Intensity | Incidence | |
| Group P | 0.8 | 0.44 | 0.003 | 0.005 | < 0.001 | < 0.001 | ||
| Group 10 | 0.8 | 0.44 | 0.014 | 0.037 | < 0.001 | < 0.001 | ||
| Group 20 | 0.003 | 0.005 | 0.014 | 0.037 | < 0.001 | < 0.001 | ||
| Group 30 | < 0.001 | < 0.001 | < 0.001 | < 0.001 | < 0.001 | < 0.001 | ||
The time of the first analgesic requirement was statistically different between group 20 and group 30. The need for pethidine was significantly lower in group 30 when compared with other groups, but was not significant between group P and group 10 or 20 [Table 4].
Table 4: Frequency of intra operative and post operative complications (Mean ± SD or n (%)
| Group complication | Group P | Group 10 | Group 20 | Group 30 | P |
|---|---|---|---|---|---|
| No complication (n - %) | 22 (73.3) | 23 (76.6) | 21 (70) | 18 (60) | 0.96 |
| Bradycardia (n - %) | 3 (10) | 1 (3.3) | 2 (6.7) | 2 (6.7) | |
| Hypotension (n - %) | 1 (3.3) | 1 (3.3) | 1 (3.3) | 2 (6.7) | |
| Urinary retention (n - %) | 1 (3.3) | 1 (3.3) | 1 (3.3) | 2 (6.7) | |
| Nausea (n - %) | 1 (3.3) | 1 (3.3) | 1 (3.3) | 2 (6.7) | |
| Vomiting (n - %) | 1 (3.3) | 1 (3.3) | 1 (3.3) | 1 (3.3) | |
| Itching (n - %) | 1 (3.3) | 2 (6.7) | 3 (10) | 3 (10) | |
| First pethidine prescription (minute) | 8.25 ± 4.1 | 8.06 ± 2.4 | 23 ± 5.6 | 35 ± 7.1 | < 0.001 |
| Pethidine dose (mg) | 39.5 ± 10.9 | 44.1 ± 10.5 | 40 ± 13.1 | 7.5 ± 3.5 | < 0.001 |
Postoperative complications had no statistically significant difference between 4 groups (P = 0.98) and there was no significant change in mean values of hemodynamic parameters during the study period.
Discussion
Our study results showed that the adding of low dose fentanyl to hyperbaric bupivacaine for spinal anesthesia in patients undergoing lower limb orthopedic surgery, reduced the incidence and severity of intraoperative and postoperative shivering and this reduction was significantly higher with the using 30 μg intrathecal fentanyl when compared with other groups (groups 20, 10, and placebo).
Previous works demonstrated that intratechal low dose fentanyl lowers the intensity of postoperative shivering after TURP surgeries under spinal anesthesia[18].
In another study Techanivate et al showed that the adding of 20 μgr Fentanyl to hyperbaric bupivacaine for spinal anesthesia in patients undergoing cesarean section diminishes the incidence and intensity of intraoperative and postoperative shivering[19]. Also Sadegh et al[21] concluded that intratecal bupivacaine combined with fentanyl is associated with a lower incidence and severity of shivering in cesarean section under spinal anesthesia, but another study by chu et al[18] revealed the combination of bupivacaine with a dose of fentanyl as low as 7.5 μg did not produce actual clinical effect and as the dose of fentanyl was increased to 12.5 μg or 15 μg the quality of surgical analgesia was better and the incidence of shivering was decreased significantly.
In the present study the need for additional analgesics (pethidine) was significantly lower in group 30 (received 30 μg fentanyl combined with bupivacaine) when compared with other groups (groups 20, 10 and placebo). Previous studies have shown that patients who had undergo cesarean section under spinal anesthesia, benefit from simultaneous administration of local anesthetics and opiates because of increased ease of surgery[22], significant increase in duration of spinal anesthesia[23] and lesser need for sedatives and analgesia post operatively[24]. The findings of the present study confirm the results of other studies for example Shahriari et al[25] showed that adding 15 μg fentanyl to 80 mg lidocaine intrathecally increased the duration of anesthesia and quality of analgesia during spinal anesthesia in women who undergo cesarean section. Also palmer and colleagues found similar results in a comparable study[26]. Jacobson et al[27] studied the effect of adding intratechal fentanyl (25 μg) to 70 mg lidocaine and showed that this will increase the quality of analgesia and may cause euphoria in patients. In our study hemodynamic parameters such as blood pressure, heart rate and blood oxygen saturation were not significantly different between four groups in addition, no case of hemodynamic instability and respiratory difficulty were seen in 4 groups. Other studies have demonstrated similar results. For example, some studies have shown that administration of 15 μg intrathecal fentanyl is not associated with respiratory depression[25,28,29]. Also this is in accordance with basic science investigations that postoperative pain relief stabilizes patient hemodynamic[30].
Fentanyl is a highly ionized, lipophilic μ- receptor agonist. When it is administered intrathecally, the unionized component is rapidly transferred into the spinal cord. The reduction of shivering in the present study may be attributable to the effect of fentanyl that was added into the subarachnoid space on the thermo – regulator and spinal effect afferent thermal inputs at the spinal cord[20]. The limitation of this study was the small sample size and the fact that we followed patients with ASA physical status I-II only for 2 h postoperatively.
Conclusion
Intrathecal bupivacaine combined with fentanyl 20 or 30 μg is associated with a lower incidence and intensity of shivering than combination of bupivacaine and 10 μg fentanyl of saline normal.
Acknowledgement:
The authors wish to sincerely thank the support of all the colleagues in Kashani Hospital Medical Center in Isfahan, Iran. Furthermore our special thanks go to the patients who actively assisted us to carry out this research. We thank the nurses at the recovery room and operating room for their contribution to the study.
Conflict of Interest:
Authors have no conflict of interests.
Authors’ Contributions
MRS has planned the study and finalized it; TF, AH, MN, MAN, DM and MRS did the statistical analysis and prepared the first version of manuscript for publish. All authors read and approved the final manuscript.
References
- 1. Chan, A.M., Ng, K.F., Tong, E.W., et al. Control of shivering under regional anesthesia in obstetric patients with tramadol. (1999) Can J Anaesth 46(3): 253-258.
- 2. Sessler, D.I., Ponte, J. Shivering during epidural anesthesia. (1990) Anesthesiology 72(5): 816-821.
- 3. Jeon, Y.T., Jeon, Y.S., Kim, Y.C., et al. Intrathecal clonidine does not reduce post-spinal shivering. (2005) Acta Anaesthesiol Scand 49(10): 1509-1513.
- 4. Macintyre, P.E., Pavlin, E.G., Dwersteg, J.F. Effect of meperidine on oxygen consumption, carbon dioxide production, and respiratory gas exchange in postanesthesia shivering. (1987) Anesth Analg 66(8): 751-755.
- 5. Piper, S.N., Fent, M.T., Rohm, K.D., et al. Urapidil does not prevent postanesthetic shivering: a dose-ranging study. (2001) Can J Anaesth 48(8): 742-747.
- 6. Tsai, Y.C., Chu, K.S. A comparison of tramadol , amitriptyline, and meperidine for postepidural anesthetic shivering in parturients. (2001) Anesth Analg 93(5): 1288-1292.
- 7. Reihanak, T., Shahrokh, N. Effect of Tramadol in Postspinal shivering in Caeserian section.
- 8. Biazzotto, C.B., Brudniewski, M., Schmidt, A.P., et al. [Perioperative hypothermia]. (2006) Rev Bras Anestesiol 56(1): 89-106.
- 9. Capogna, G., Celleno, D. Improving epidural anesthesia during cesarean section: causes of maternal discomfort or pain during surgery. (1994) Int J Obstet Anesth 3(3): 149-152.
- 10. Braga Ade, F., Braga, F.S., Poterio, G.M., et al. Sufentanil added to hyperbaric bupivacaine for subarachnoid block in Caesarean section. (2003) Eur J Anaesthesiol 20(8): 631-635.
- 11. De Witte, J., Sessler, D.I. Perioperative shivering: physiology and pharmacology. (2002) Anesthesiology 96(2): 467-484.
- 12. Leighton, B.L., DeSimone, C.A., Norris, M.C., et al. Intrathecal narcotics for labor revisited: the combination of fentanyl and morphine intrathecally provides rapid onset and profound, prolonged prolonged analgesia. (1989) Anesth Analg 69(1): 122-125.
- 13. Rueben, S.S., Dunn, S.M., Dupart, K.M., et al. An intrathecal fentanyl dose-response study in lower extremity revascularization procedures. (1994) Anesthesiology 81(6): 1371-1375.
- 14. Obara, M., Sawamura, S., Satoh, Y., et al. The effect of intrathecal fentanyle added to hyperbaric bupivacaine for cesarean section. (2003) Masui 52(4): 378-382.
- 15. Belzarena, S.D. Clinical effects of intrathecally administered fentanyl in patients undergoing cesarean section. (1992) Anesth Analg 74(5): 653-657.
- 16. Hunt, C.O., Naulty, J.S., Bader, A.M., et al. Perioperative analgesia with subarachnoid fentanyl- bupivacaine for cesarean delivery. (1989) Anesthesiology 71(4): 535-540.
- 17. Dahlgern, G., Hultstrand, C., Jakobsson, J., et al. Intrathecal sufentanyl, fentanyl, or placebo added to bupivacaine for cesarean section. (1997) Anesth Analg 85(6): 1288-1293.
- 18. Chow, T.C., Cho, P.H. The influence of small dose intrathecal fentanyl on shivering during transurethral resection of prostate under spinal anesthesia. (1994) Acta Anaesthesiol Sin 32(3): 165-170.
- 19. Techanivate, A., Urusopone, P., Kiatgungwangliam, P., et al. Intratechal fentanyl in spinal anesthesia for appendectomy. (2004) J Med Assoc Thai 87(5): 525-530.
- 20. Techanivate, A., Rodanant, O., Tachawattanwisel, W., et al. Intratechal fentanyl for prevention of shivering in cesarean section. (2005) J Med Assoc Thai 88(9): 1214-1221.
- 21. Sadegh, A., Tazeh-Kand, N.F., Eslami, B. Intrathecal fentanyl for prevention of shivering in spinal anesthesia in cesarean section. (2012) Med J Islam Repub Iran 26(2): 85-89.
- 22. Dahl, J.B., Jeppesen, I.S., Jorgensen, H., et al. Intraoperative and postoperative analgesic efficacy and adverse effects of intrathecal opioids in patients undergoing cesarean section with spinal anesthesia: a qualitative and quantitative systematic review of randomized controlled trials. (1999) Anesthesiology 91(6): 1919-1927.
- 23. Hunt, C.O., Naulty, J.S., Bader, A.M., et al. Perioperative analgesia with subarachnoid fentanyl-bupivacaine for cesarean delivery. (1989) Anesthesiology 71(4): 535-540.
- 24. Graham, D., Russel, I. Double blind study to assess the analgesic sparing effect of 0.3 mg diamorphine given intrathecally at caesarean section. (1995) Int J Obs Anesth 4(3): 179-180.
- 25. Shahriari, A., Khooshideh, M. Intrathecal fentanyl added to lidocaine for Cesarean delivery under spinal anesthesia—a randomised clinical trial. (2007) Middle East J Anesthesiol 19(2): 397-406.
- 26. Palmer, C.M., Voulgaropoulos, D., Alves, D. Subarachnoid fentanyl augments lidocaine spinal anesthesia for cesarean delivery. (1995) Reg Anesth Sep 20(5): 389-394.
- 27. Jacobson, L., Chabal, C., Brody, M.C., et al. A comparison of the effects of intrathecal fentanyl and lidocaine on established postamputation stump pain. (1990) Pain 40(2): 137-141.
- 28. Hunt, C.O., Naulty, J.S., Bader, A.M., et al. Perioperative analgesia with subarachnoid fentanyl-bupivacaine for cesarean delivery. (1989) Anesthesiology 71(4): 535-540.
- 29. Shende, D., Cooper, G.M., Bowden, M.I. The influence of intrathecal fentanyl on the characteristics of subarachnoid block for caesarean section. (1998) Anaesthesia 53(7): 706-710.
- 30. Ronald D.Miller., Robert, W.Hurely., Jamie, D.Murphy., et al. Millers Anesthesia, Postoperative pains , eighth edition. (2014) Lseverchurchill Livingston 98: 2976.










